Department of Thoracic Surgery, University Hospital OWL of the University Bielefeld, campus Bielefeld-Bethel, Bielefeld, Germany.
Department of Internal Medicine and Gastroenterology, University Hospital OWL of the University Bielefeld, campus Bielefeld-Bethel, Bielefeld, Germany.
Eur J Med Res. 2021 Feb 8;26(1):19. doi: 10.1186/s40001-021-00488-9.
Diaphragmatic lesions as a result of blunt or penetrating trauma are challenging to detect in the initial trauma setting. This is especially true when diaphragmatic trauma is part of a polytrauma. Complications of undetected diaphragmatic defects with incarcerating bowel are rare, but as in our patient can be serious.
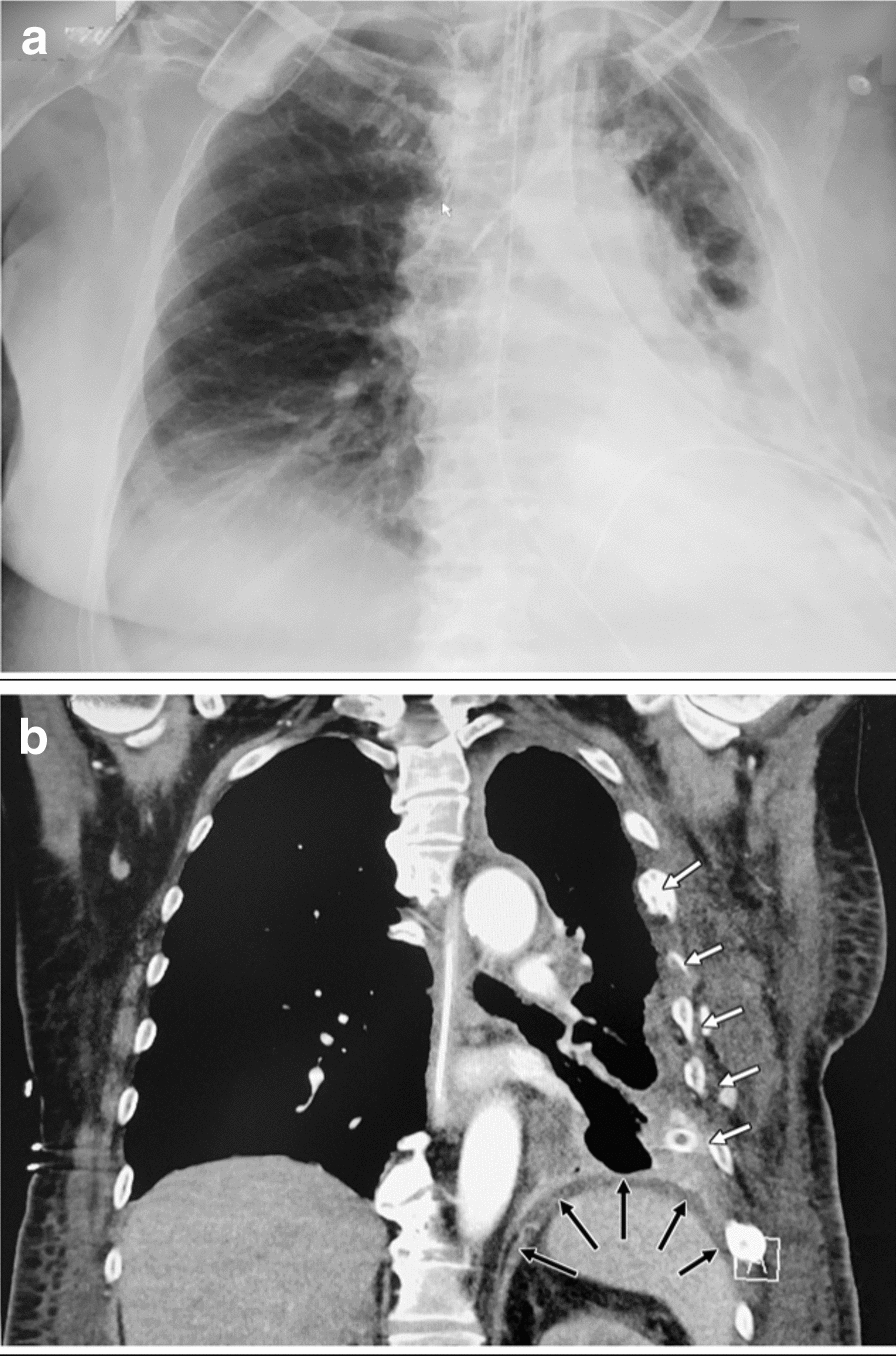
A 57-year-old female presented to the Emergency Room of our Hospital in a critical condition with 3 days of increasing abdominal pain. The initial clinical examination showed peritonism with tinkling peristaltic bowel sounds of mechanical obstruction. A thoraco-abdominal CT scan demonstrated colon prolapsed through the left diaphragmatic center with a large sero-pneumothorax under tension. As the patient was hemodynamically increasingly unstable with developing septic shock, an emergency laparotomy was performed. After retraction of the left colon, which had herniated through a defect of the tendinous center of the left diaphragm and was perforated due to transmural ischemia, large amounts of feces and gas discharged from the left thorax. A left hemicolectomy resulting in a Hartmann-type procedure was performed. A fully established pleural empyema required meticulous debridement and lavage conducted via the 7-10 cm in diameter phrenic opening followed by a diaphragmatic defect reconstruction. Due to pneumonia and recurring pleural empyema redo-debridement of the left pleural space via thoracotomy were required. The patient was discharged on day 56. A thorough history of possible trauma revealed a bicycle-fall trauma 7 months prior to this hospitalization with a surgically stabilized fracture of the left femur and conservatively treated fractures of ribs 3-9 on the left side.
This is the first report on a primarily established empyema at the time of first surgical intervention for feco-pneumothorax secondary to delayed diagnosed diaphragmatic rupture following abdomino-thoracic blunt trauma with colic perforation into the pleural space, requiring repetitive surgical debridement in order to control local and systemic sepsis. Thorough investigation should always be undertaken in cases of blunt abdominal and thoracic trauma to exclude diaphragmatic injury in order to avoid post-traumatic complications.
钝性或穿透性创伤导致的膈肌损伤在初始创伤情况下难以检测。当膈肌损伤是多发伤的一部分时尤其如此。未发现伴有嵌顿肠的膈肌缺陷的并发症很少见,但在我们的患者中可能很严重。
一名 57 岁女性因腹痛逐渐加重 3 天而被紧急送往我院急诊科。最初的临床检查显示有腹膜炎,肠鸣音亢进,机械性梗阻。胸部和腹部 CT 扫描显示结肠通过左膈肌中心疝出,张力下有大量气胸。由于患者血流动力学越来越不稳定,出现感染性休克,因此进行了紧急剖腹手术。在回缩疝出的左结肠后,发现由于穿透性缺血导致的左膈肌腱性中心缺陷穿孔,大量粪便和气体从左侧胸腔排出。进行了左半结肠切除术,导致 Hartmann 型手术。完全形成的脓胸需要通过 7-10cm 直径的膈孔进行仔细清创和灌洗,然后进行膈肌缺陷重建。由于肺炎和复发性脓胸,需要通过开胸手术再次对左侧胸腔进行清创。患者于第 56 天出院。对可能的创伤进行全面的病史回顾发现,在本次住院前 7 个月,该患者曾发生过自行车跌倒创伤,导致左侧股骨手术固定骨折,左侧肋骨 3-9 保守治疗骨折。
这是首例报告,即初次手术干预治疗因钝性胸腹创伤导致的结肠穿孔进入胸腔,随后发生延迟诊断的膈肌破裂,导致继发性的粪气胸,在控制局部和全身败血症方面需要重复进行手术清创。对于钝性腹部和胸部创伤,应始终进行彻底的调查,以排除膈肌损伤,避免创伤后并发症。