Department of Medicine, Donald and Barbara Zucker School of Medicine at Hofstra/Northwell, Northwell Health, Hempstead, New York, USA.
Institute of Health Innovations and Outcomes Research, Feinstein Institutes for Medical Research, Northwell Health, Manhasset, New York, USA.
BMJ Open. 2021 Feb 8;11(2):e042965. doi: 10.1136/bmjopen-2020-042965.
To describe the pattern of hydroxychloroquine use and examine the association between hydroxychloroquine use and clinical outcomes arising from changes in the US Food and Drug Administration (FDA)'s recommendation during the coronavirus disease 2019 (COVID-19) pandemic.
A retrospective cross-sectional analysis.
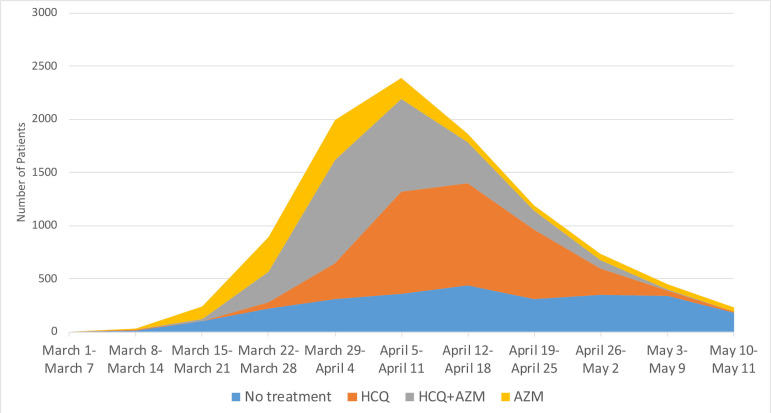
We included hospitalised adult patients at Northwell Health hospitals with confirmed COVID-19 infections between 1 March 2020 and 11 May 2020. We categorised changes in the FDA's recommendation as pre-FDA approval (1 March 2020-27 March 2020), FDA approval (28 March 2020-23 April 2020), and FDA warning (24 April 2020-11 May 2020). The hydroxychloroquine-treated group received at least one dose within 48 hours of hospital admission.
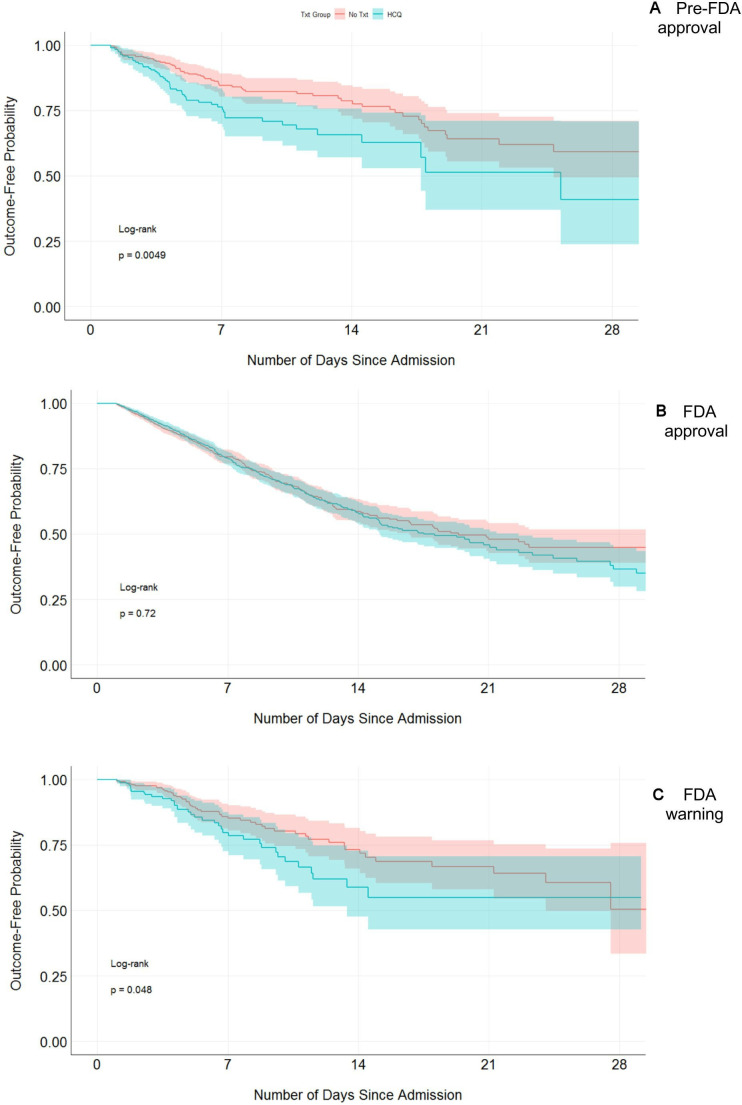
A composite of intubation and inpatient death.
The percentages of patients who were treated with hydroxychloroquine were 192/2202 (8.7%) pre-FDA approval, 2902/6741 (43.0%) FDA approval, and 176/1066 (16.5%) FDA warning period (p<0.001). Using propensity score matching, there was a higher rate of the composite outcome among patients treated with hydroxychloroquine (49/192, 25.5%) compared with no hydroxychloroquine (66/384, 17.2%) in the pre-FDA approval period (p=0.03) but not in the FDA approval period (25.5% vs 22.6%, p=0.08) or the FDA warning (21.0% vs 15.1%, p=0.11) periods. Coincidently, there was an increase in number of patients with COVID-19 and disease severity during the FDA approval period (24.1% during FDA approval vs 21.4% during pre-FDA approval period had the composite outcome). Hydroxychloroquine use was associated with increased odds of the composite outcome during the pre-FDA approval period (OR=1.65 (95% CI 1.09 to 2.51)) but not during the FDA approval (OR=1.17 (95% CI 0.99 to 1.39)) and FDA warning (OR=1.50 (95% CI 0.94 to 2.39)) periods.
Hydroxychloroquine use was associated with adverse clinical outcomes only during the pre-FDA approval period but not during the FDA approval and warning periods, even after adjusting for concurrent changes in the percentage of patients with COVID-19 treated with hydroxychloroquine and the number (and disease severity) of hospitalised patients with COVID-19 infections.
描述羟氯喹使用模式,并考察美国食品药品监督管理局(FDA)在新冠肺炎大流行期间建议改变后,羟氯喹使用与临床结局之间的关联。
回顾性横断面分析。
我们纳入了 2020 年 3 月 1 日至 5 月 11 日期间在诺斯韦尔健康医院住院的确诊新冠肺炎感染的成年患者。我们将 FDA 建议的改变分为 FDA 批准前(2020 年 3 月 1 日至 3 月 27 日)、FDA 批准后(2020 年 3 月 28 日至 4 月 23 日)和 FDA 警告后(2020 年 4 月 24 日至 5 月 11 日)。羟氯喹治疗组在入院后 48 小时内至少接受一剂羟氯喹治疗。
插管和住院死亡的复合结局。
在 FDA 批准前、FDA 批准后和 FDA 警告期间,接受羟氯喹治疗的患者比例分别为 192/2202(8.7%)、2902/6741(43.0%)和 176/1066(16.5%)(p<0.001)。使用倾向评分匹配后,在 FDA 批准前期间,接受羟氯喹治疗的患者(49/192,25.5%)比未接受羟氯喹治疗的患者(66/384,17.2%)复合结局发生率更高(p=0.03),但在 FDA 批准后(25.5% vs 22.6%,p=0.08)或 FDA 警告后(21.0% vs 15.1%,p=0.11)期间无差异。巧合的是,在 FDA 批准期间,COVID-19 患者数量和疾病严重程度增加(FDA 批准期间 24.1%的患者发生复合结局,而 FDA 批准前为 21.4%)。在 FDA 批准前期间,羟氯喹的使用与复合结局的发生几率增加相关(OR=1.65(95%CI 1.09 至 2.51)),但在 FDA 批准后(OR=1.17(95%CI 0.99 至 1.39))和 FDA 警告后(OR=1.50(95%CI 0.94 至 2.39))期间无差异。
羟氯喹的使用仅与 FDA 批准前期间的不良临床结局相关,而与 FDA 批准和警告期间无关,即使在调整了同时接受羟氯喹治疗的 COVID-19 患者比例以及 COVID-19 感染住院患者数量(和疾病严重程度)的变化后也如此。