Ziółkowska Lidia, Mazurkiewicz Łukasz, Petryka Joanna, Kowalczyk-Domagała Monika, Boruc Agnieszka, Bieganowska Katarzyna, Ciara Elżbieta, Piekutowska-Abramczuk Dorota, Śpiewak Mateusz, Miśko Jolanta, Marczak Magdalena, Brzezińska-Rajszys Grażyna
Department of Cardiology, The Children's Memorial Health Institute, 04-730 Warsaw, Poland.
CMR Unit, Department of Cardiomyopathies, National Institute of Cardiology, 04-628 Warsaw, Poland.
J Clin Med. 2021 Feb 8;10(4):650. doi: 10.3390/jcm10040650.
The most efficient risk stratification algorithms are expected to deliver robust and indefectible identification of high-risk children with hypertrophic cardiomyopathy (HCM). Here we compare algorithms for risk stratification in primary prevention in HCM children and investigate whether novel indices of biatrial performance improve these algorithms.
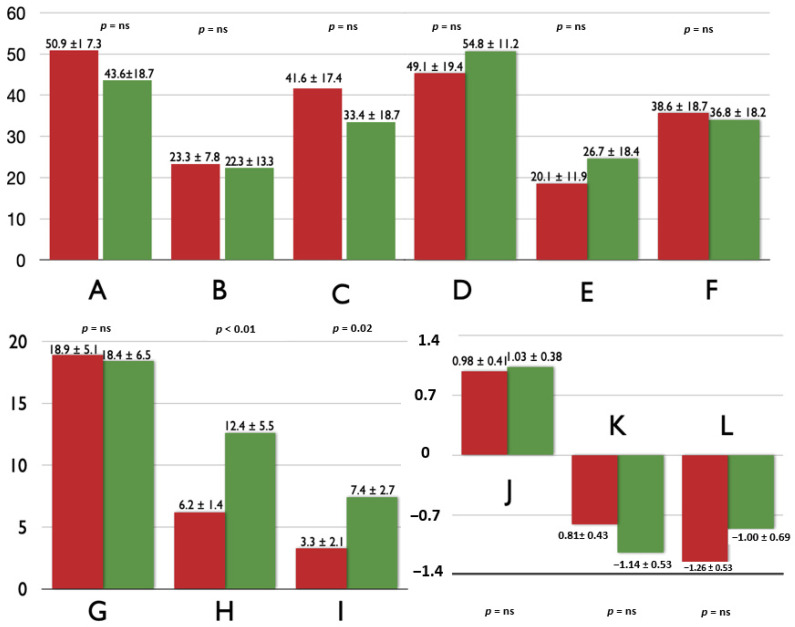
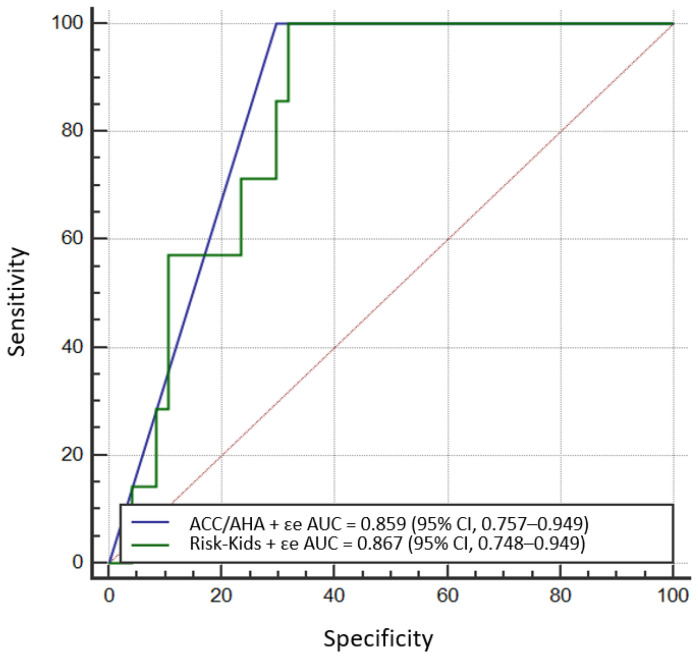
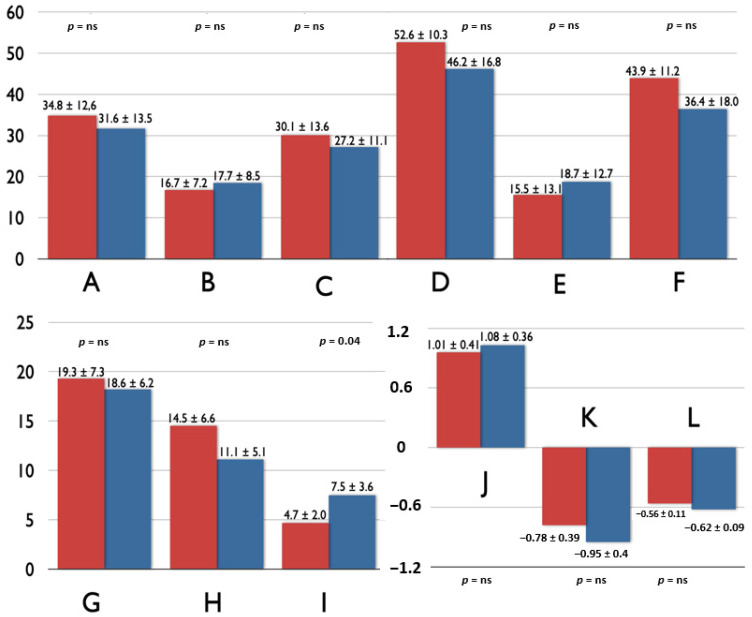
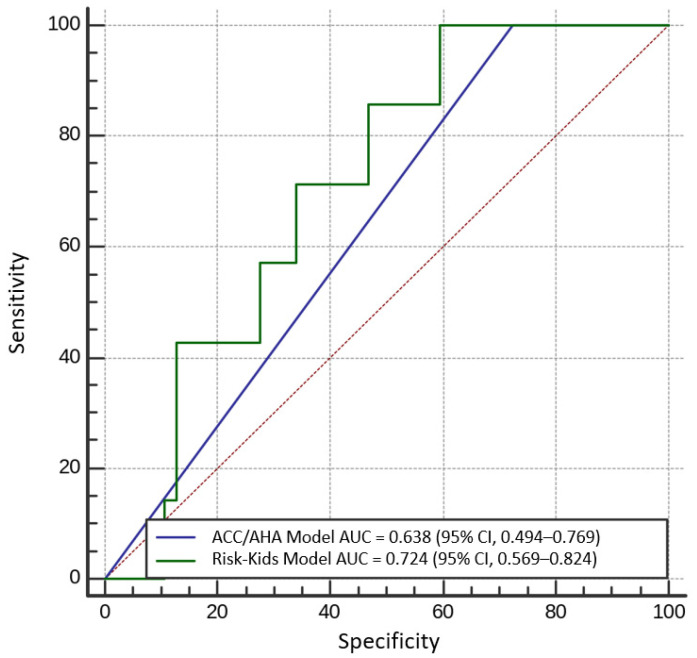
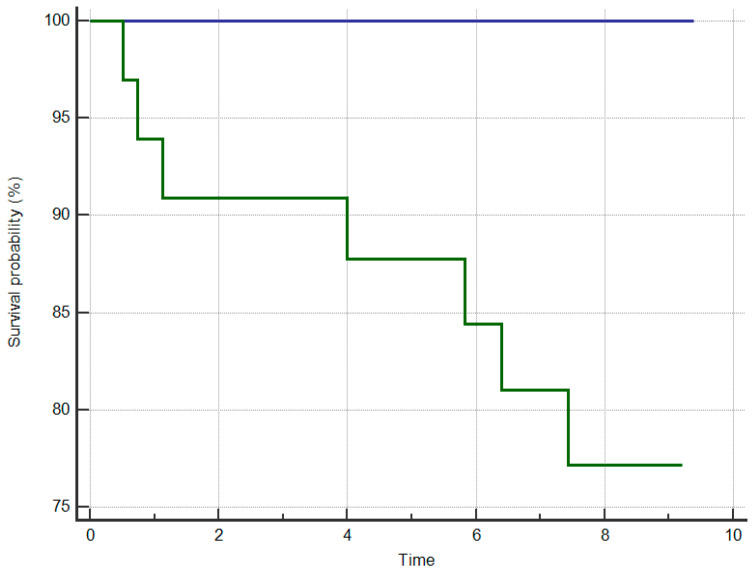
The endpoints were defined as sudden cardiac death, resuscitated cardiac arrest, or appropriate implantable cardioverter-defibrillator discharge. We examined the prognostic utility of classic American College of Cardiology/American Heart Association (ACC/AHA) risk factors, the novel HCM Risk-Kids score and the combination of these with indices of biatrial dynamics. The study consisted of 55 HCM children (mean age 12.5 ± 4.6 years, 69.1% males); seven had endpoints (four deaths, three appropriate ICD discharges). A strong trend (DeLong = 0.08) was observed towards better endpoint identification performance of the HCM Risk-Kids Model compared to the ACC/AHA strategy. Adding the atrial conduit function component significantly improved the prediction capabilities of the AHA/ACC Model (DeLong = 0.01) and HCM Risk-Kids algorithm (DeLong = 0.04).
The new HCM Risk-Kids individualised algorithm and score was capable of identifying high-risk children with very good accuracy. The inclusion of one of the atrial dynamic indices improved both risk stratification strategies.
最有效的风险分层算法应能可靠且无误地识别肥厚型心肌病(HCM)高危儿童。在此,我们比较HCM儿童一级预防中的风险分层算法,并研究双房功能新指标是否能改善这些算法。
终点定义为心源性猝死、心脏骤停复苏或植入式心律转复除颤器(ICD)恰当放电。我们检验了美国心脏病学会/美国心脏协会(ACC/AHA)经典危险因素、新的HCM Risk-Kids评分以及将这些与双房动力学指标相结合的预后效用。该研究纳入了55例HCM儿童(平均年龄12.5±4.6岁,69.1%为男性);7例出现终点事件(4例死亡,3例ICD恰当放电)。与ACC/AHA策略相比,观察到HCM Risk-Kids模型在终点识别性能方面有明显更好的趋势(德龙检验=0.08)。加入心房管道功能成分显著改善了AHA/ACC模型(德龙检验=0.01)和HCM Risk-Kids算法(德龙检验=0.04)的预测能力。
新的HCM Risk-Kids个体化算法和评分能够以很高的准确性识别高危儿童。纳入一项心房动力学指标改善了两种风险分层策略。