Mölzer Christine, Heissigerova Jarmila, Wilson Heather M, Kuffova Lucia, Forrester John V
Institute of Medical Sciences, University of Aberdeen, Aberdeen, United Kingdom.
Department of Ophthalmology, First Faculty of Medicine, Charles University and General University Hospital in Prague, Prague, Czechia.
Front Immunol. 2021 Jan 25;11:608377. doi: 10.3389/fimmu.2020.608377. eCollection 2020.
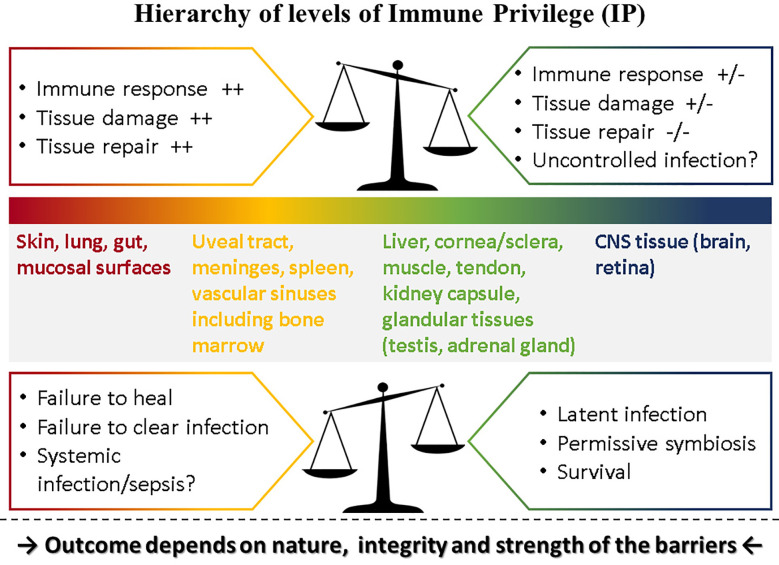
Immune privilege (IP), a term introduced to explain the unpredicted acceptance of allogeneic grafts by the eye and the brain, is considered a unique property of these tissues. However, immune responses are modified by the tissue in which they occur, most of which possess IP to some degree. The eye therefore displays a spectrum of IP because it comprises several tissues. IP as originally conceived can only apply to the retina as it contains few tissue-resident bone-marrow derived myeloid cells and is immunologically shielded by a sophisticated barrier - an inner vascular and an outer epithelial barrier at the retinal pigment epithelium. The vascular barrier comprises the vascular endothelium and the glia limitans. Immune cells do not cross the blood-retinal barrier (BRB) despite two-way transport of interstitial fluid, governed by tissue oncotic pressure. The BRB, and the blood-brain barrier (BBB) mature in the neonatal period under signals from the expanding microbiome and by 18 months are fully established. However, the adult eye is susceptible to intraocular inflammation (uveitis; frequency ~200/100,000 population). Uveitis involving the retinal parenchyma (posterior uveitis, PU) breaches IP, while IP is essentially irrelevant in inflammation involving the ocular chambers, uveal tract and ocular coats (anterior/intermediate uveitis/sclerouveitis, AU). Infections cause ~50% cases of AU and PU but infection may also underlie the pathogenesis of immune-mediated "non-infectious" uveitis. Dysbiosis accompanies the commonest form, HLA-B27-associated AU, while latent infections underlie BRB breakdown in PU. This review considers the pathogenesis of uveitis in the context of IP, infection, environment, and the microbiome.
免疫赦免(IP)这一术语最初用于解释眼睛和大脑对同种异体移植物的意外接受,被认为是这些组织的独特属性。然而,免疫反应会受到其发生组织的影响,大多数组织在某种程度上都具有免疫赦免特性。眼睛由于由多种组织构成,因此呈现出一系列免疫赦免情况。最初所设想的免疫赦免仅适用于视网膜,因为视网膜中几乎没有组织驻留的骨髓来源的髓样细胞,并且在视网膜色素上皮处被一个复杂的屏障——内部血管屏障和外部上皮屏障——免疫隔离。血管屏障由血管内皮和神经胶质界膜组成。尽管组织胶体渗透压控制着间质液的双向运输,但免疫细胞不会穿过血视网膜屏障(BRB)。血视网膜屏障和血脑屏障(BBB)在新生儿期,在不断扩展的微生物群发出的信号作用下成熟,并在18个月时完全建立。然而,成年眼睛易患眼内炎症(葡萄膜炎;发病率约为200/10万人口)。涉及视网膜实质的葡萄膜炎(后葡萄膜炎,PU)会破坏免疫赦免,而免疫赦免在涉及眼房、葡萄膜和眼外膜的炎症(前/中间葡萄膜炎/巩膜葡萄膜炎,AU)中基本无关紧要。感染导致约50%的AU和PU病例,但感染也可能是免疫介导的“非感染性”葡萄膜炎发病机制的基础。共生失调伴随着最常见的形式,即HLA - B27相关的AU,而潜伏感染是PU中血视网膜屏障破坏的基础。本综述在免疫赦免、感染、环境和微生物群的背景下探讨葡萄膜炎的发病机制。