Hamada Akira, Soh Junichi, Mitsudomi Tetsuya
Division of Thoracic Surgery, Department of Surgery, Kindai University Faculty of Medicine, Osaka-Sayama, Japan.
Transl Lung Cancer Res. 2021 Jan;10(1):555-562. doi: 10.21037/tlcr-20-453.
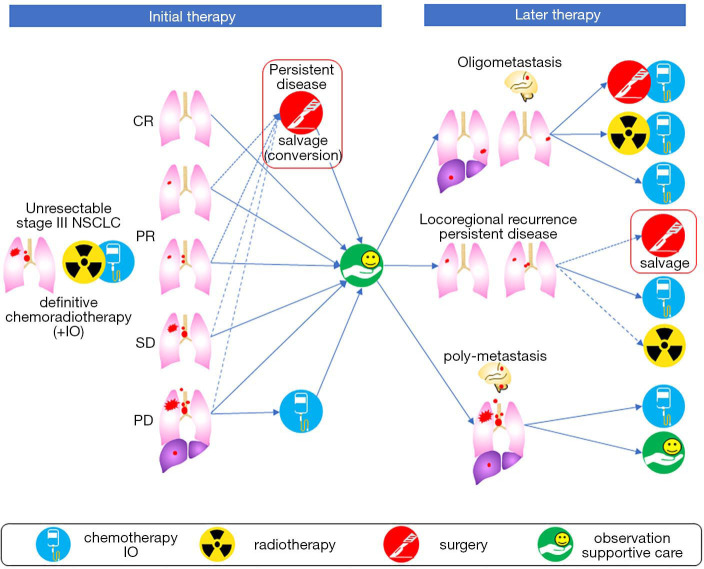
Definitive chemoradiotherapy (CRT) has been a standard of care for patients with unresectable stage III non-small cell lung cancer (NSCLC). However, locoregional recurrence occurs in about 30% of patients after definitive CRT. Recently, the addition of durvalumab as maintenance therapy has shown to improve the outcome of these patients. However, locoregional recurrence will still remain. "Salvage surgery" has been performed to achieve local control in clinical practice, although its clinical significance is unclear. In this review, we define salvage surgery as lung resection for local control of the tumor which was not planned initially, after failure or insufficient treatment effect of the initial CRT for locally advanced cancer and evaluated nine studies to gain some insights on its role in the treatment of lung cancer. The time from radiotherapy (RT) to salvage surgery varied considerably (range, 3 to 282 weeks). Salvage surgery was performed for persistent disease (47%) and locoregional recurrence (52%). Lobectomy (63%) and mediastinal lymph node dissections (90%) were the most common procedures. However, the rate of pneumonectomy was higher in salvage surgery (28%) compared to that in lung resection in general. The median morbidity was 41% (range, 15% to 62%) and the mortality was 4% (range, 0 to 11%) which appeared acceptable. The median recurrence-free survival and overall survival (OS) after salvage surgery ranged from 10 to 22 months and 13 to 76 months, respectively. Favorable prognostic factors of salvage surgery were longer period from RT to salvage surgery and radiological downstaging. The pathological response was also prognostic, although this information cannot be obtained preoperatively. We conclude that salvage surgery can be considered especially for those with late local recurrence or those with the metabolic response. Given the condition where phase III trials are difficult, the accumulation of real-world evidence in a prospective fashion will be necessary.
确定性放化疗(CRT)一直是不可切除的III期非小细胞肺癌(NSCLC)患者的标准治疗方案。然而,约30%的患者在确定性CRT后会出现局部区域复发。最近,添加度伐利尤单抗作为维持治疗已显示可改善这些患者的预后。然而,局部区域复发仍会存在。在临床实践中已进行“挽救性手术”以实现局部控制,尽管其临床意义尚不清楚。在本综述中,我们将挽救性手术定义为在局部晚期癌症的初始CRT失败或治疗效果不佳后,为局部控制肿瘤而进行的肺切除术,该肿瘤最初并未计划切除,并评估了九项研究以了解其在肺癌治疗中的作用。从放疗(RT)到挽救性手术的时间差异很大(范围为3至282周)。挽救性手术用于持续性疾病(47%)和局部区域复发(52%)。肺叶切除术(63%)和纵隔淋巴结清扫术(90%)是最常见的手术方式。然而,与一般肺切除术相比,挽救性手术中的全肺切除术发生率更高(28%)。中位发病率为41%(范围为15%至62%),死亡率为4%(范围为0至11%),这似乎是可以接受的。挽救性手术后的中位无复发生存期和总生存期(OS)分别为10至22个月和13至76个月。挽救性手术的有利预后因素是从RT到挽救性手术的时间更长以及影像学降期。病理反应也具有预后意义,尽管术前无法获得此信息。我们得出结论,挽救性手术尤其适用于局部晚期复发或有代谢反应的患者。鉴于开展III期试验困难的情况,以前瞻性方式积累真实世界证据将是必要的。