Li Jia, Liu Dongwei, Liu Zhangsuo
Department of Nephrology, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, China.
Research Institute of Nephrology, Zhengzhou University, Zhengzhou, China.
Front Med (Lausanne). 2021 Jan 25;7:549. doi: 10.3389/fmed.2020.00549. eCollection 2020.
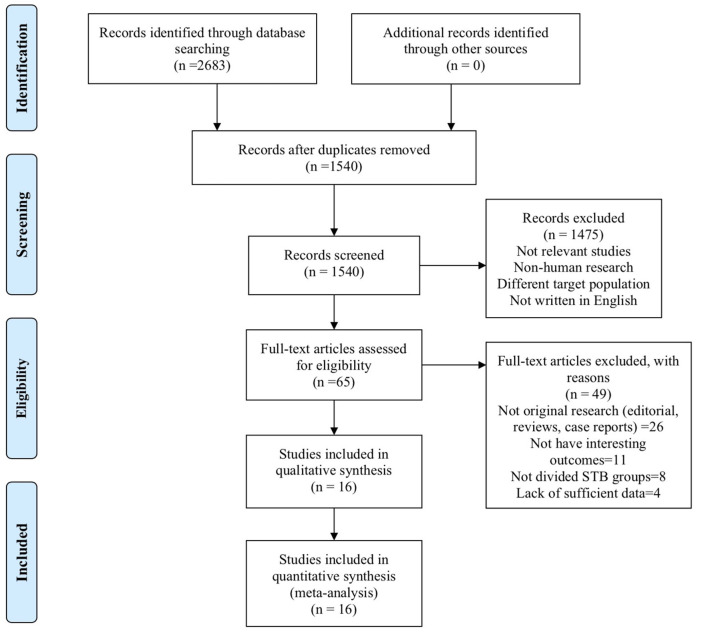
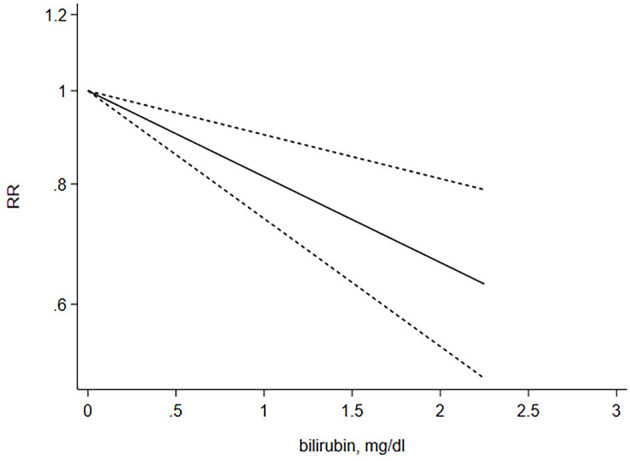
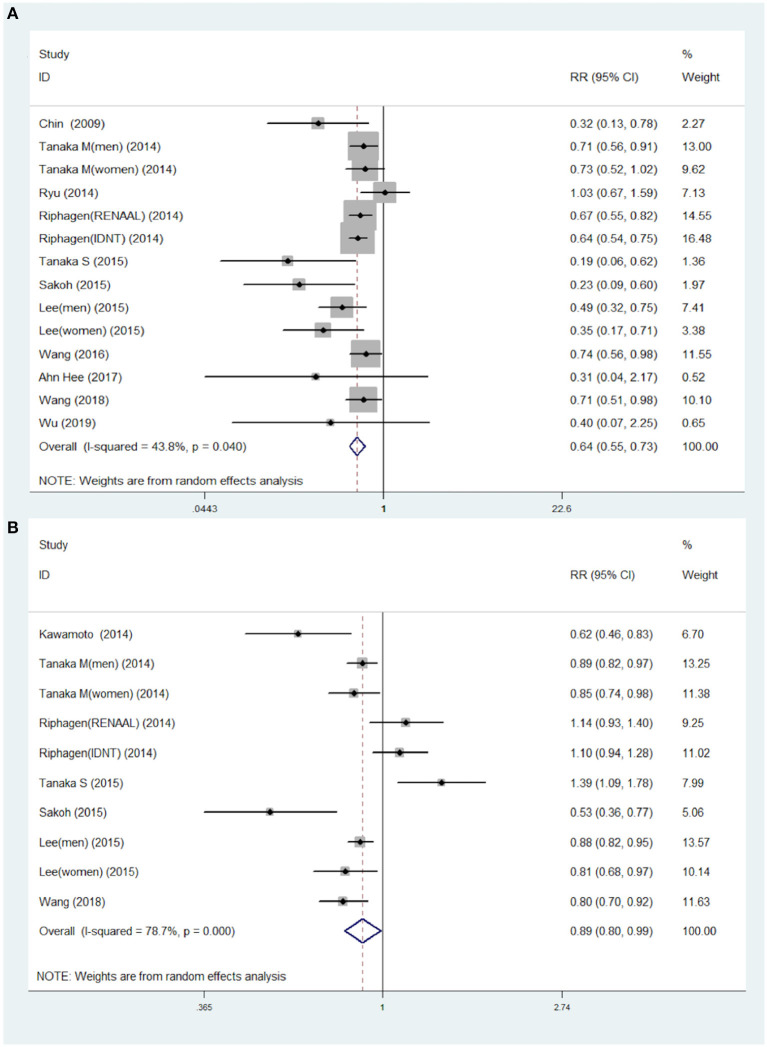
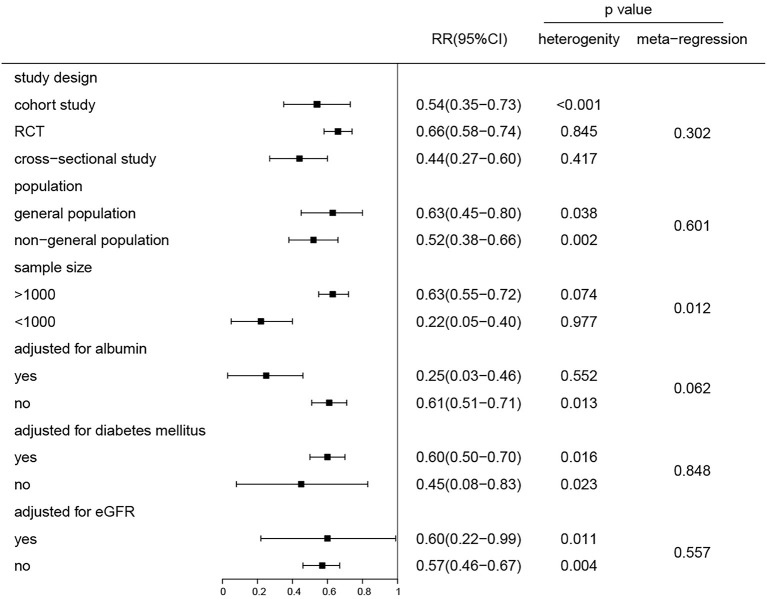
Previous studies have suggested that serum total bilirubin (STB) levels are associated with heightened chronic kidney disease (CKD) and mortality in both the general population and nephropathy patients. However, these results remain inconsistent. The aim of our study was to investigate whether STB was a predictor for progression of CKD and mortality by meta-analysis. We performed a systematic literature search in PubMed, Web of Science, MEDLINE, EMBASE, Google Scholar, and Cochrane Library's database up to June 30, 2019. Pooled risk ratios (RR) and corresponding 95% confidence intervals (CI) were extracted for the highest vs. lowest category STB levels within the physiological range, and a random-effects model was applied to calculate the dose-response relationships. A pooled hazard ratio (HR) was used to investigate the association between STB levels and mortality in dialysis patients. A total of 16 studies, wherein participants were followed from 21 months to 7 years, were eligible for inclusion in the study. For the categorized STB, 11 studies with 41,188 participants were identified and analyzed. Patients with the highest STB levels were associated with a lower risk of CKD (RR = 0.64; 95% CI 0.55-0.73) compared to those with the lowest STB levels. Furthermore, based on seven studies, a pooled RR of 0.89, 95% CI (0.80-0.99) was observed for the continuous STB levels (per 0.2 mg/dL increase). Four studies that included 51,764 participants illustrated that there was no association between STB levels and all-cause mortality (HR = 0.77; 95% CI 0.42-1.41). A prominent negative linear relationship (X = 14.70; = 0.0001) was found between STB levels and risk of CKD. Subgroup analyses showed that there were no significant differences in the subgroup adjustment factor except for sample size. Elevated STB levels within a physiological range are associated with lower risk of CKD regardless of the study characteristics and coincide with a liner dose-response relationship. However, whether high STB levels are a protective factor against mortality remains inconclusive. Large-scale randomized controlled trails are needed to target STB levels for predicting renal outcomes.
先前的研究表明,在普通人群和肾病患者中,血清总胆红素(STB)水平与慢性肾脏病(CKD)的加重及死亡率相关。然而,这些结果仍不一致。我们研究的目的是通过荟萃分析探究STB是否为CKD进展及死亡率的预测指标。我们在PubMed、Web of Science、MEDLINE、EMBASE、谷歌学术以及Cochrane图书馆数据库中进行了系统的文献检索,检索截至2019年6月30日。提取生理范围内STB水平最高组与最低组的合并风险比(RR)及相应的95%置信区间(CI),并应用随机效应模型计算剂量反应关系。采用合并风险比(HR)来研究STB水平与透析患者死亡率之间的关联。共有16项研究符合纳入标准,这些研究对参与者的随访时间为21个月至7年。对于分类的STB,共识别并分析了11项研究,涉及41,188名参与者。与STB水平最低的患者相比,STB水平最高的患者患CKD的风险较低(RR = 0.64;95% CI 0.55 - 0.73)。此外,基于7项研究,连续STB水平(每增加0.2mg/dL)的合并RR为0.89,95% CI(0.80 - 0.99)。四项涉及51,764名参与者的研究表明,STB水平与全因死亡率之间无关联(HR = 0.77;95% CI 0.42 - 1.41)。发现STB水平与CKD风险之间存在显著的负线性关系(X = 14.70;P = 0.0001)。亚组分析表明除样本量外,亚组调整因素无显著差异。生理范围内STB水平升高与较低的CKD风险相关,与研究特征无关,且符合线性剂量反应关系。然而,高STB水平是否为死亡率的保护因素仍无定论。需要大规模随机对照试验以针对STB水平来预测肾脏结局。