Anesthesia and Intensive Care, Fatebenefratelli Hospital, Piazza Principessa Clotilde, 3, 20121, Milan, Italy.
Department of Statistics and Quantitative Methods, University of Milano-Bicocca, Via degli Arcimboldi, 8, 20126, Milan, Italy.
World J Surg. 2021 Apr;45(4):928-939. doi: 10.1007/s00268-020-05940-1. Epub 2021 Feb 11.
Previous Enhanced Recovery After Surgery (ERAS®) studies have not always taken into account that ERAS interventions depend on baseline covariates and that several confounding variables affect the composite outcomes.
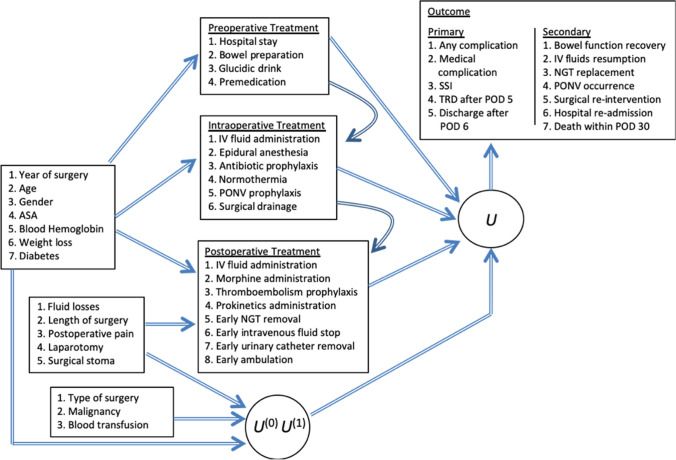
A causal latent variable model is proposed to analyze data obtained prospectively concerning 1261 patients undergoing elective colorectal surgery within the ERAS protocol. Primary outcomes (composite of any complication, surgical site infection, medical complications, early ready for discharge (TRD), early actual discharge) and secondary outcomes (composite of late bowel function recovery, IV fluid resumption, nasogastric tube replacement, postoperative nausea and vomiting, re-intervention, re-admission, death) are considered along with their multiple dimensions.
Concerning the primary outcomes, our results evidence three subpopulations of patients: one with probable good outcome, one with possibly prolonged TRD and discharge without complications, and the other one with probable complications and prolonged TRD and discharge. Epidural anesthesia, waiving surgical drainage, and early ambulation, IV fluid stop and urinary catheter removal act favorably, while preoperative hospital stay and blood transfusion act negatively. Concerning the secondary outcomes our results evidence two subpopulations of patients: one with high probability of good outcome and one with high probability of complications. Epidural anesthesia, waiving surgical drainage, early ambulation and IV fluid stop act favorably, while blood transfusion acts negatively also with respect to these secondary outcomes.
The multivariate causal latent class two-parameter logistic model, a modern statistical method overcoming drawbacks of traditional models to estimate the average causal effects on the treated, allows us to disentangle subpopulations of patients and to evaluate ERAS interventions.
之前的术后加速康复(ERAS®)研究并未充分考虑到 ERAS 干预措施取决于基线协变量,并且有几个混杂变量会影响综合结果。
提出了一个因果潜在变量模型,用于分析在 ERAS 方案下接受择期结直肠手术的 1261 例患者前瞻性获得的数据。主要结果(任何并发症、手术部位感染、医疗并发症、早期准备出院(TRD)、早期实际出院的复合结果)和次要结果(迟发性肠功能恢复、静脉补液恢复、鼻胃管更换、术后恶心和呕吐、再次干预、再次入院、死亡的复合结果)以及它们的多个维度都被考虑在内。
关于主要结果,我们的结果显示了患者的三个亚群:一个可能有良好结局的亚群,一个可能 TRD 延长且无并发症出院的亚群,另一个可能出现并发症且 TRD 延长和出院的亚群。硬膜外麻醉、放弃手术引流、早期活动、停止静脉补液和拔除导尿管均有利,而术前住院时间和输血则不利。关于次要结果,我们的结果显示了患者的两个亚群:一个有较高可能性出现良好结局的亚群,另一个有较高可能性出现并发症的亚群。硬膜外麻醉、放弃手术引流、早期活动和停止静脉补液均有利,而输血也对这些次要结果产生负面影响。
多变量因果潜在类别二参数逻辑模型是一种现代统计方法,可以克服传统模型的缺点,估计对治疗组的平均因果效应,从而使我们能够区分患者亚群并评估 ERAS 干预措施。