Gastrointestinal Surgery, Nottingham Digestive Diseases Centre, National Institute of Health Research (NIHR) Nottingham Biomedical Research Centre, Nottingham University Hospitals NHS Trust and University of Nottingham, Queen's Medical Centre, Nottingham NG7 2UH, United Kingdom.
World J Gastroenterol. 2018 Jan 28;24(4):519-536. doi: 10.3748/wjg.v24.i4.519.
To analyse the effect of mechanical bowel preparation no mechanical bowel preparation on outcome in patients undergoing elective colorectal surgery.
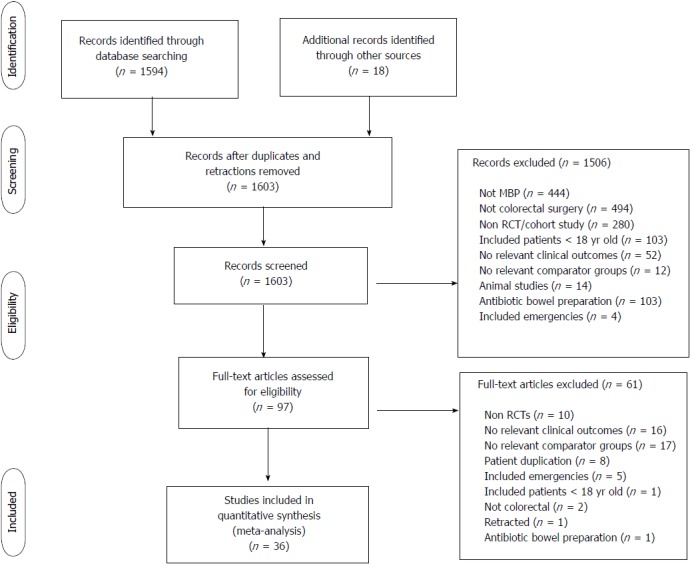
Meta-analysis of randomised controlled trials and observational studies comparing adult patients receiving mechanical bowel preparation with those receiving no mechanical bowel preparation, subdivided into those receiving a single rectal enema and those who received no preparation at all prior to elective colorectal surgery.
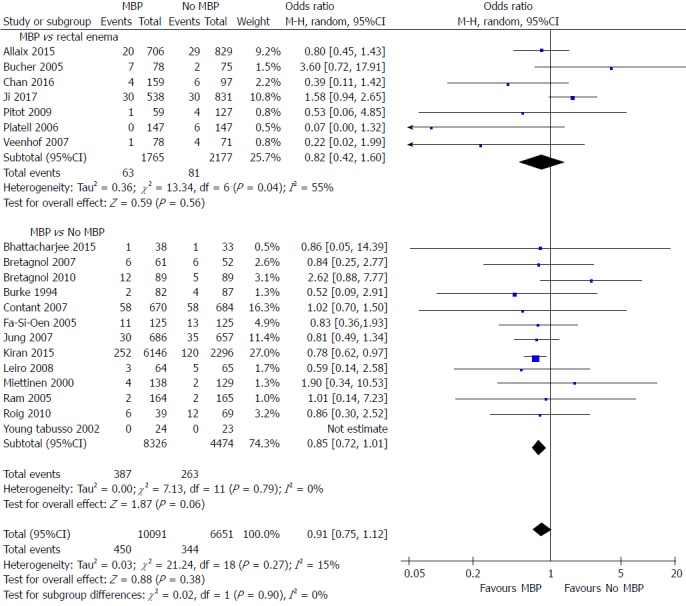
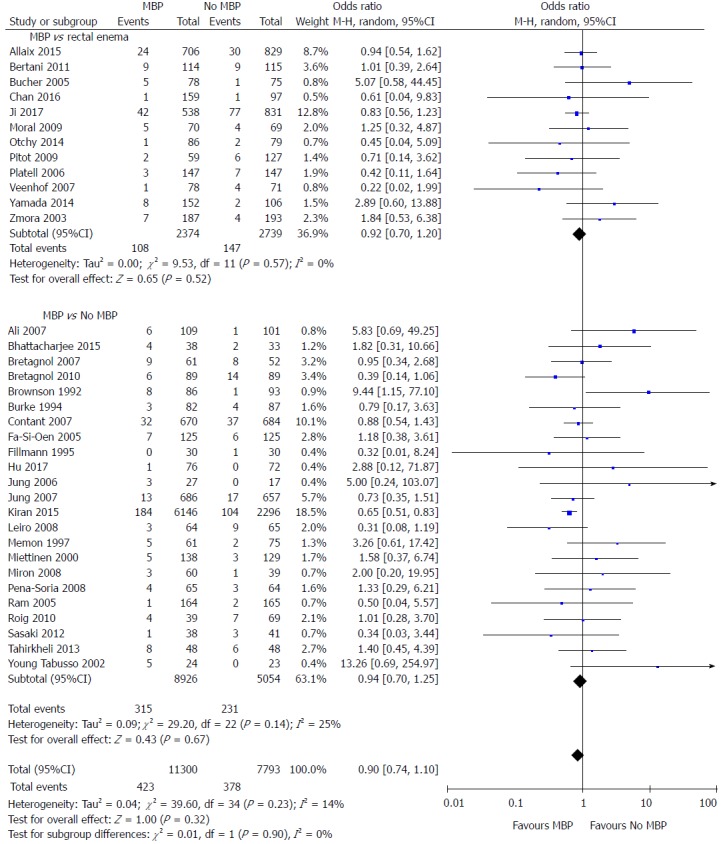
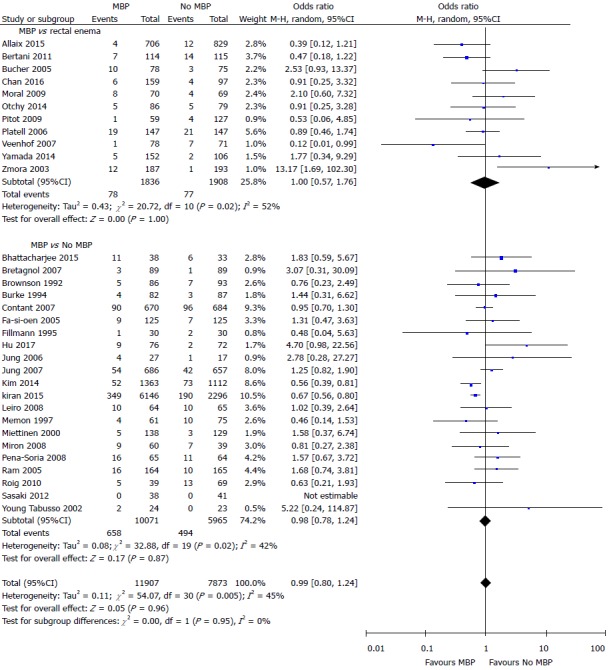
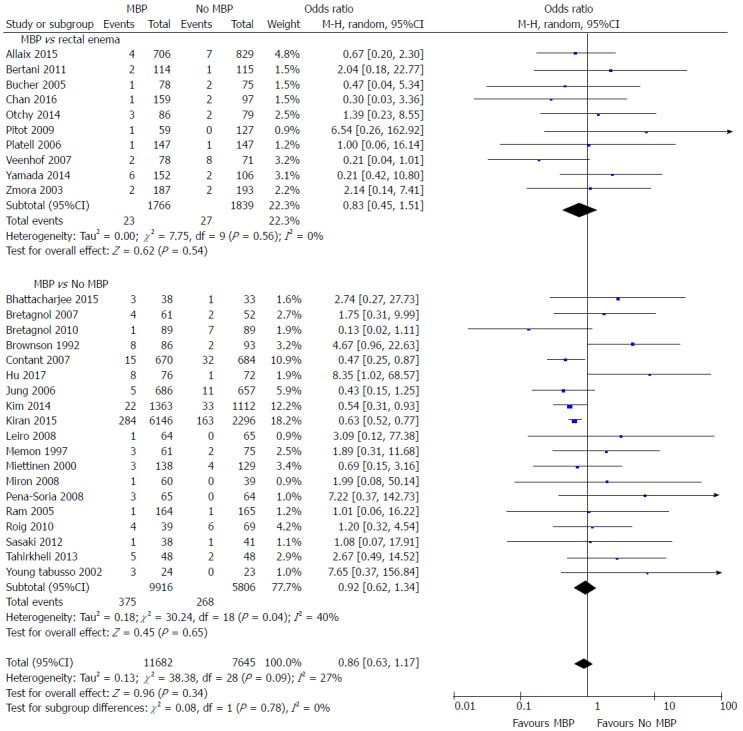
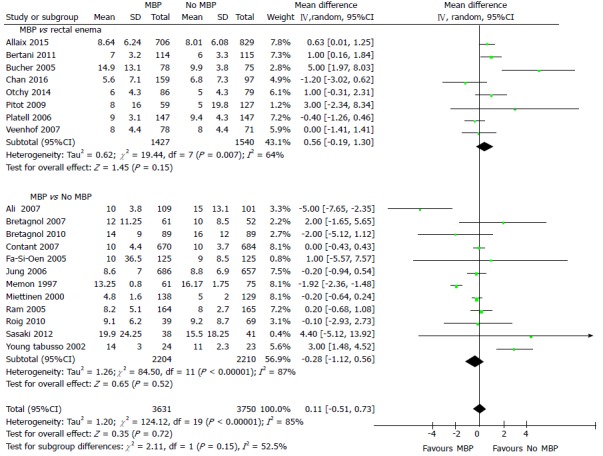
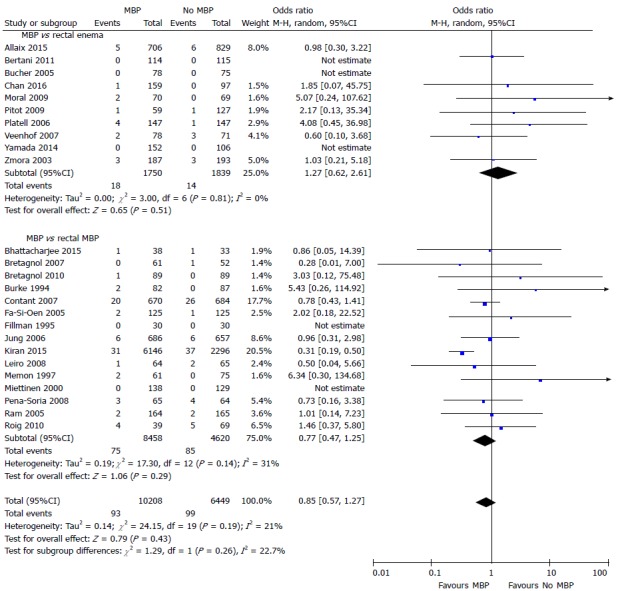
A total of 36 studies (23 randomised controlled trials and 13 observational studies) including 21568 patients undergoing elective colorectal surgery were included. When all studies were considered, mechanical bowel preparation was not associated with any significant difference in anastomotic leak rates (OR = 0.90, 95%CI: 0.74 to 1.10, = 0.32), surgical site infection (OR = 0.99, 95%CI: 0.80 to 1.24, = 0.96), intra-abdominal collection (OR = 0.86, 95%CI: 0.63 to 1.17, = 0.34), mortality (OR = 0.85, 95%CI: 0.57 to 1.27, = 0.43), reoperation (OR = 0.91, 95%CI: 0.75 to 1.12, = 0.38) or hospital length of stay (overall mean difference 0.11 d, 95%CI: -0.51 to 0.73, = 0.72), when compared with no mechanical bowel preparation, nor when evidence from just randomized controlled trials was analysed. A sub-analysis of mechanical bowel preparation absolutely no preparation or a single rectal enema similarly revealed no differences in clinical outcome measures.
In the most comprehensive meta-analysis of mechanical bowel preparation in elective colorectal surgery to date, this study has suggested that the use of mechanical bowel preparation does not affect the incidence of postoperative complications when compared with no preparation. Hence, mechanical bowel preparation should not be administered routinely prior to elective colorectal surgery.
分析择期结直肠手术中进行机械肠道准备与不进行机械肠道准备对患者结局的影响。
对比较接受机械肠道准备与不接受机械肠道准备的成年患者的随机对照试验和观察性研究进行荟萃分析,分为接受单次直肠灌肠和术前完全不准备的患者。
共纳入 36 项研究(23 项随机对照试验和 13 项观察性研究),包括 21568 例择期结直肠手术患者。当考虑所有研究时,机械肠道准备与吻合口漏发生率(OR = 0.90,95%CI:0.74 至 1.10, = 0.32)、手术部位感染(OR = 0.99,95%CI:0.80 至 1.24, = 0.96)、腹腔积液(OR = 0.86,95%CI:0.63 至 1.17, = 0.34)、死亡率(OR = 0.85,95%CI:0.57 至 1.27, = 0.43)、再次手术(OR = 0.91,95%CI:0.75 至 1.12, = 0.38)或住院时间(总体平均差异 0.11 天,95%CI:-0.51 至 0.73, = 0.72)相比,接受机械肠道准备并不优于不接受机械肠道准备,即使仅分析随机对照试验的证据也是如此。对机械肠道准备 绝对不准备或单次直肠灌肠的亚分析同样表明,临床结局指标无差异。
在迄今为止对择期结直肠手术中机械肠道准备最全面的荟萃分析中,本研究表明与不准备相比,使用机械肠道准备不会影响术后并发症的发生率。因此,择期结直肠手术前不应常规给予机械肠道准备。