Sumitomo Dainippon Pharma Oncology, Inc., Cambridge, MA, USA.
Nuventra Inc., Durham, NC, USA.
Pharmacol Res Perspect. 2021 Feb;9(1):e00722. doi: 10.1002/prp2.722.
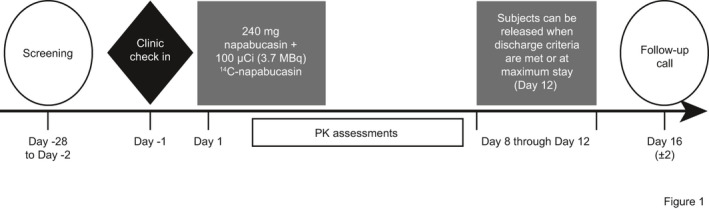
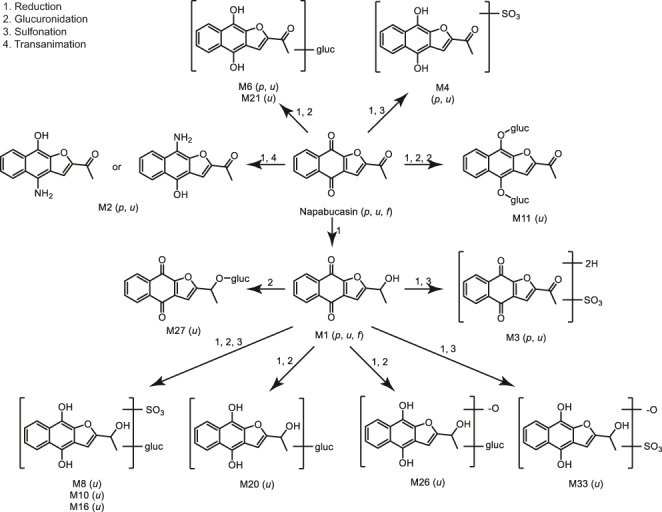
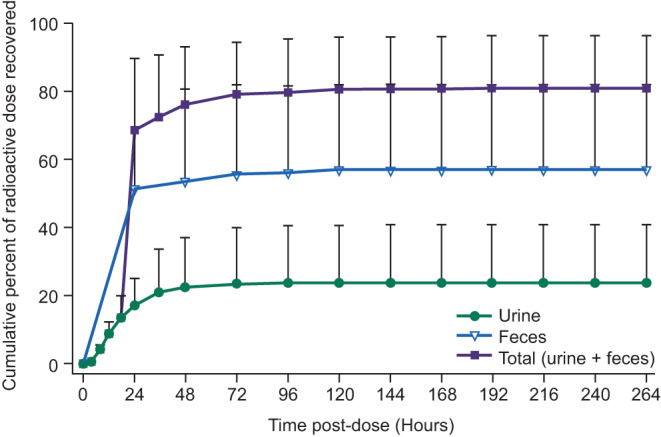
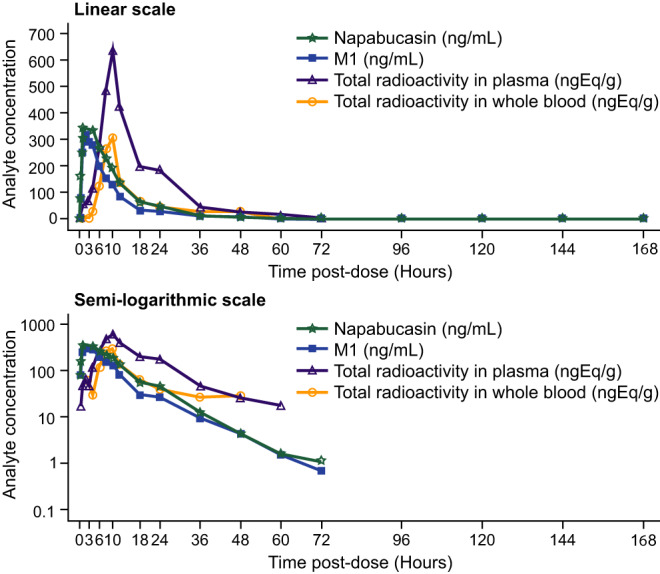
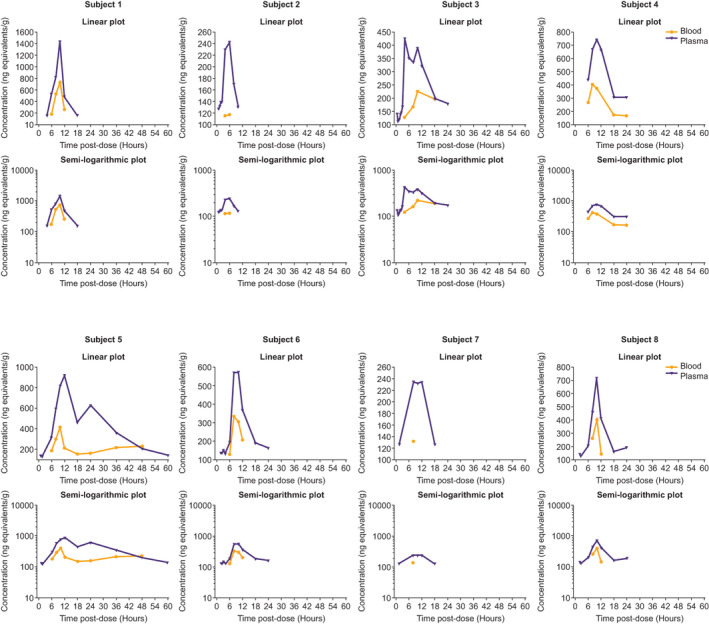
This phase 1, open-label study assessed C-napabucasin absorption, metabolism, and excretion, napabucasin pharmacokinetics, and napabucasin metabolites (primary objectives); safety/tolerability were also evaluated. Eight healthy males (18-45 years) received a single oral 240-mg napabucasin dose containing ~100 μCi C-napabucasin. Napabucasin was absorbed and metabolized to dihydro-napabucasin (M1; an active metabolite [12.57-fold less activity than napabucasin]), the sole major circulating metabolite (median time to peak concentration: 2.75 and 2.25 h, respectively). M1 plasma concentration versus time profiles generally mirrored napabucasin; similar arithmetic mean half-lives (7.14 and 7.92 h, respectively) suggest M1 formation was rate limiting. Napabucasin systemic exposure (per C and AUC) was higher than M1. The total radioactivity (TRA) whole blood:plasma ratio (AUC : 0.376; C : 0.525) indicated circulating drug-related compounds were essentially confined to plasma. Mean TRA recovery was 81.1% (feces, 57.2%; urine, 23.8%; expired air, negligible). Unlabeled napabucasin and M1 recovered in urine accounted for 13.9% and 11.0% of the dose (sum similar to urine TRA recovered); apparent renal clearance was 8.24 and 7.98 L/h. No uniquely human or disproportionate metabolite was quantified. Secondary glucuronide and sulfate conjugates were common urinary metabolites, suggesting napabucasin was mainly cleared by reductive metabolism. All subjects experienced mild treatment-emergent adverse events (TEAEs), the majority related to napabucasin. The most commonly reported TEAEs were gastrointestinal disorders. There were no clinically significant laboratory, vital sign, electrocardiogram, or physical examination changes. Napabucasin was absorbed, metabolized to M1 as the sole major circulating metabolite, and primarily excreted via feces. A single oral 240-mg dose was generally well tolerated.
这是一项 I 期、开放标签研究,旨在评估 C-纳巴昔布的吸收、代谢和排泄、纳巴昔布的药代动力学以及纳巴昔布代谢物(主要目标);还评估了安全性/耐受性。8 名健康男性(18-45 岁)接受了单次口服 240mg 纳巴昔布,其中含有约 100μCi C-纳巴昔布。纳巴昔布被吸收并代谢为二氢-纳巴昔布(M1;一种活性代谢物[比纳巴昔布活性低 12.57 倍]),是唯一主要的循环代谢物(峰浓度中位时间:分别为 2.75 和 2.25 小时)。M1 的血浆浓度-时间曲线大致反映了纳巴昔布;相似的算术平均半衰期(分别为 7.14 和 7.92 小时)表明 M1 的形成是限速步骤。纳巴昔布的全身暴露量(按 C 和 AUC 计)高于 M1。全血:血浆比(AUC:0.376;C:0.525)表明循环药物相关化合物基本上局限于血浆。平均 TRA 回收率为 81.1%(粪便,57.2%;尿液,23.8%;呼气,可忽略不计)。未标记的纳巴昔布和 M1 在尿液中的回收量占剂量的 13.9%和 11.0%(总和与尿液 TRA 回收量相似);表观肾清除率分别为 8.24 和 7.98 L/h。未定量到任何独特的人类或不成比例的代谢物。次级葡萄糖醛酸和硫酸盐缀合物是常见的尿液代谢物,表明纳巴昔布主要通过还原代谢清除。所有受试者均经历了轻度的治疗后出现的不良事件(TEAEs),大多数与纳巴昔布相关。报告最常见的 TEAEs 是胃肠道疾病。实验室、生命体征、心电图或体检均无临床显著变化。纳巴昔布被吸收,代谢为 M1,是唯一主要的循环代谢物,主要通过粪便排泄。单次口服 240mg 剂量通常具有良好的耐受性。