Huttin Olivier, Kobayashi Masatake, Ferreira João Pedro, Coiro Stefano, Bozec Erwan, Selton-Suty Christine, Filipetti Laura, Lamiral Zohra, Rossignol Patrick, Zannad Faiez, Girerd Nicolas
Université de Lorraine, Centre d'Investigations Cliniques-Plurithématique, Inserm1433, CHRU Nancy, Inserm DCAC, and F-CRIN INI-CRCT (Cardiovascular and Renal Clinical Trialists), INSERM CHU de Nancy, Institut Lorrain du Cœur et des Vaisseaux Louis Mathieu, 4 Rue du Morvan, 54500 Vandoeuvre lès, Nancy, France.
Service de Cardiologie, Institut Lorrain du Cœur et des Vaisseaux, Centre Hospitalier Universitaire de Nancy, Nancy, France.
ESC Heart Fail. 2021 Apr;8(2):1700-1705. doi: 10.1002/ehf2.13203. Epub 2021 Feb 12.
Biomarkers reflecting myocardial fibrosis and inflammation have been individually associated with left ventricular hypertrophy (LVH) and diastolic dysfunction (DD). However, the added value of a fibrosis-inflammation multimarker approach in a populational setting is yet to be studied. We evaluated the value of a multimarker approach to detect LVH and DD in a large population-based cohort.
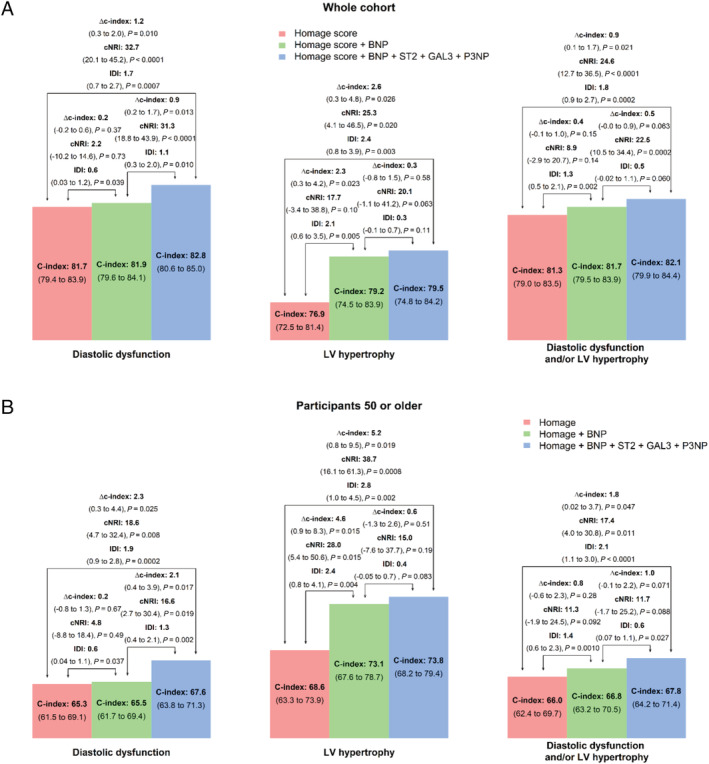
In a prespecified analysis (BioSe-PreIC study) of the 4th visit of the STANISLAS cohort (1705 subjects, 47 ± 14 years, 47.4% men), we evaluated the ability of brain natriuretic peptide (BNP), Galectin-3 (GAL3), N-terminal propeptide of procollagen type III (P3NP), and soluble ST2 to predict LVH (LV mass > 116/100 g/m for men/women) and DD using discrimination (C-index) and reclassification analysis (NRI). Participants with LVH and/or DD had significantly higher levels of BNP, GAL3, and ST2. Overall, the predictive value of clinical variables for LVH and/or DD was good (C-index ranging from 0.76 to 0.82) and the addition of BNP, Gal3, P3NP, and ST2 moderately but significantly improved predictive value (delta C-index = 0.03, P = 0.03 for LVH and 0.01, P = 0.01 for DD) and reclassification (NRI = 25.3, P = 0.02 for LVH and NRI = 32.7 for DD, P < 0.0001). Gal3, P3NP, and ST2 significantly improved predictive value (delta C-index = 0.01, P = 0.01) and reclassification (NRI = 31.3, P < 0.0001) for DD of top of clinical variables and BNP.
As the measurement of Gal3, P3NP, and ST2 results in marginal (even if significant) increase in the prediction of DD/LVH on top of routine evaluation, their systematic use should not be promoted in unselected healthy individuals to screen for preclinical DD. Further research is needed to determine whether a more personalized medicine approach combing proteomic and clinical scoring can amplify the added value of biomarkers to identify preclinical DD.
反映心肌纤维化和炎症的生物标志物已分别与左心室肥厚(LVH)和舒张功能障碍(DD)相关。然而,在人群环境中,纤维化 - 炎症多标志物方法的附加价值尚待研究。我们评估了一种多标志物方法在大型基于人群的队列中检测LVH和DD的价值。
在斯坦尼斯拉斯队列第四次随访(1705名受试者,47±14岁,47.4%为男性)的预先指定分析(BioSe - PreIC研究)中,我们评估了脑钠肽(BNP)、半乳糖凝集素 - 3(GAL3)、Ⅲ型前胶原氨基端前肽(P3NP)和可溶性ST2预测LVH(男性/女性左心室质量>116/100 g/m)和DD的能力,采用判别分析(C指数)和重新分类分析(NRI)。患有LVH和/或DD的参与者的BNP、GAL3和ST2水平显著更高。总体而言,临床变量对LVH和/或DD的预测价值良好(C指数范围为0.76至0.82),添加BNP、Gal3、P3NP和ST2适度但显著提高了预测价值(LVH的C指数增量=0.03,P = 0.03;DD 的C指数增量=0.01,P = 0.01)和重新分类(LVH的NRI = 25.3,P = 0.02;DD的NRI = 32.7,P < 0.0001)。Gal3、P3NP和ST2显著提高了临床变量和BNP之上对DD的预测价值(C指数增量=0.01,P = 0.01)和重新分类(NRI = 31.3,P < 0.0001)。
由于测量Gal3、P3NP和ST2在常规评估之上对DD/LVH预测的增加幅度很小(即使有显著增加),在未经选择的健康个体中不应该推广将它们用于筛查临床前DD。需要进一步研究以确定结合蛋白质组学和临床评分的更个性化医疗方法是否可以扩大生物标志物识别临床前DD的附加价值。