Department of Hematologic Oncology and Blood Disorders, Levine Cancer Institute, Atrium Health, Charlotte, NC.
Division of Biostatistics, Institute for Heath and Equity and.
Blood Adv. 2021 Feb 23;5(4):975-983. doi: 10.1182/bloodadvances.2020003654.
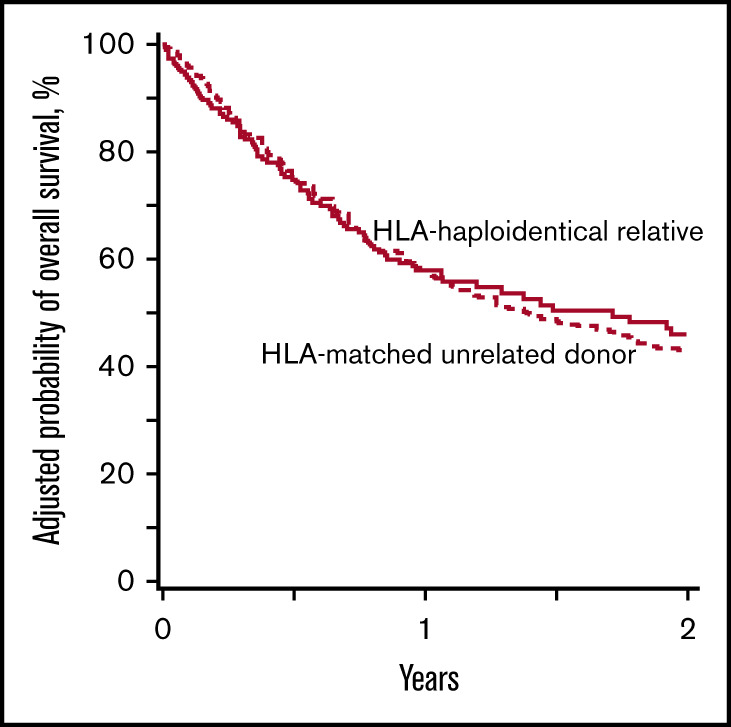
We compared outcomes in 603 patients with myelodysplastic syndrome (MDS) after HLA-haploidentical relative (n = 176) and HLA-matched unrelated (n = 427) donor hematopoietic cell transplantation (HCT) from 2012 to 2017, using the Center for International Blood and Marrow Transplant Research database. All transplantations used reduced-intensity conditioning regimens. Total-body irradiation plus cyclophosphamide and fludarabine was the predominant regimen for HLA-haploidentical relative donor HCT, and graft-versus-host disease (GVHD) prophylaxis was uniformly posttransplantation cyclophosphamide, calcineurin inhibitor, and mycophenolate. Fludarabine with busulfan or melphalan was the predominant regimen for HLA-matched unrelated donor HCT, and GVHD prophylaxis was calcineurin inhibitor with mycophenolate or methotrexate. Results of multivariate analysis revealed higher relapse (hazard ratio [HR], 1.56; P = .0055; 2-year relapse rate, 48% vs 33%) and lower disease-free survival (DFS) rates after HLA-haploidentical relative donor HCT (HR, 1.29; P = .042; 2-year DFS, 29% vs 36%). However, overall survival (OS) rates did not differ between donor type (HR, 0.94; P = .65; 2-year OS, 46% for HLA-haploidentical and 44% for HLA-matched unrelated donor HCT) because of mortality associated with chronic GVHD. Acute grade 2 to 4 GVHD (HR, 0.44; P < .0001) and chronic GVHD (HR, 0.36; P < .0001) were lower after HLA-haploidentical relative donor HCT. By 2 years, probability of death resulting from chronic GVHD was lower after HLA-haploidentical relative compared with HLA-matched unrelated donor HCT (6% vs 21%), negating any potential survival advantage from better relapse control. Both donor types extend access to transplantation for patients with MDS; strategies for better relapse control are desirable for HLA-haploidentical relative donor HCT, and effective GVHD prophylaxis regimens are needed for unrelated donor HCT.
我们比较了 2012 年至 2017 年间,603 例骨髓增生异常综合征(MDS)患者接受 HLA 单倍体相合亲缘(n=176)和 HLA 匹配无关供体(n=427)造血细胞移植(HCT)后的结果,这些数据来自国际血液和骨髓移植研究中心数据库。所有移植均采用强度降低的预处理方案。全身体照射加环磷酰胺和氟达拉滨是 HLA 单倍体相合亲缘供者 HCT 的主要方案,移植物抗宿主病(GVHD)预防措施均为环磷酰胺、钙调神经磷酸酶抑制剂和霉酚酸。氟达拉滨联合白消安或马法兰是 HLA 匹配无关供者 HCT 的主要方案,GVHD 预防措施为钙调神经磷酸酶抑制剂联合霉酚酸或甲氨蝶呤。多因素分析结果显示,HLA 单倍体相合亲缘供者 HCT 后复发率较高(危险比[HR],1.56;P=.0055;2 年复发率为 48% vs 33%),无病生存(DFS)率较低(HR,1.29;P=.042;2 年 DFS 率为 29% vs 36%)。然而,由于慢性 GVHD 导致的死亡率,两种供体类型之间的总生存(OS)率没有差异(HR,0.94;P=.65;2 年 OS 率,HLA 单倍体为 46%,HLA 匹配无关为 44%)。HLA 单倍体相合亲缘供者 HCT 后急性 2-4 级 GVHD(HR,0.44;P<.0001)和慢性 GVHD(HR,0.36;P<.0001)发生率较低。2 年内,HLA 单倍体相对 HLA 匹配无关供体 HCT 后因慢性 GVHD 导致的死亡率较低(6% vs 21%),否定了更好的复发控制带来的任何潜在生存优势。这两种供体类型都为 MDS 患者提供了移植的机会;对于 HLA 单倍体相合亲缘供者 HCT,需要更好的复发控制策略,对于无关供者 HCT,需要有效的 GVHD 预防方案。