Department of Neurosurgery, University Hospital Salzburg, Paracelsus Medical University Salzburg, Ignaz-Harrer-Str. 79, A-5020, Salzburg, Austria.
University Institute of Neuroradiology, University Hospital Salzburg, Paracelsus Medical University Salzburg, Ignaz-Harrer-Str. 79, 5020, Salzburg, Austria.
Acta Neurochir (Wien). 2021 May;163(5):1355-1364. doi: 10.1007/s00701-021-04755-w. Epub 2021 Feb 13.
Stereoelectroencephalography (SEEG) allows the identification of deep-seated seizure foci and determination of the epileptogenic zone (EZ) in drug-resistant epilepsy (DRE) patients. We evaluated the accuracy and treatment-associated morbidity of frameless VarioGuide® (VG) neuronavigation-guided depth electrode (DE) implantations.
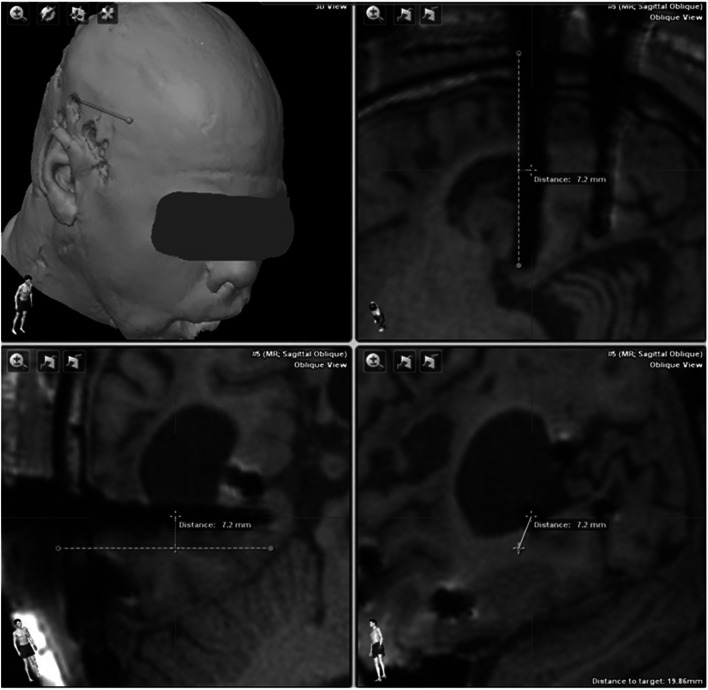
We retrospectively identified all consecutive adult DRE patients, who underwent VG-neuronavigation DE implantations, between March 2013 and April 2019. Clinical data were extracted from the electronic patient charts. An interdisciplinary team agreed upon all treatment decisions. We performed trajectory planning with iPlan® Cranial software and DE implantations with the VG system. Each electrode's accuracy was assessed at the entry (EP), the centre (CP) and the target point (TP). We conducted correlation analyses to identify factors associated with accuracy.
The study population comprised 17 patients (10 women) with a median age of 32.0 years (range 21.0-54.0). In total, 220 DEs (median length 49.3 mm, range 25.1-93.8) were implanted in 21 SEEG procedures (range 3-16 DEs/surgery). Adequate signals for postoperative SEEG were detected for all but one implanted DEs (99.5%); in 15/17 (88.2%) patients, the EZ was identified and 8/17 (47.1%) eventually underwent focus resection. The mean deviations were 3.2 ± 2.4 mm for EP, 3.0 ± 2.2 mm for CP and 2.7 ± 2.0 mm for TP. One patient suffered from postoperative SEEG-associated morbidity (i.e. conservatively treated delayed bacterial meningitis). No mortality or new neurological deficits were recorded.
The accuracy of VG-SEEG proved sufficient to identify EZ in DRE patients and associated with a good risk-profile. It is a viable and safe alternative to frame-based or robotic systems.
立体脑电图(SEEG)可识别深部致痫灶并确定耐药性癫痫(DRE)患者的致痫区(EZ)。我们评估了无框架 VarioGuide®(VG)神经导航引导深度电极(DE)植入术的准确性和与治疗相关的发病率。
我们回顾性地确定了 2013 年 3 月至 2019 年 4 月期间所有接受 VG 神经导航 DE 植入的成年 DRE 患者。从电子病历中提取临床数据。一个跨学科团队就所有治疗决策达成一致。我们使用 iPlan®Cranial 软件进行轨迹规划,并使用 VG 系统进行 DE 植入。评估每个电极的准确性在入口点(EP)、中心点(CP)和靶点(TP)。我们进行了相关性分析,以确定与准确性相关的因素。
研究人群包括 17 名患者(10 名女性),中位年龄为 32.0 岁(范围 21.0-54.0)。总共在 21 例 SEEG 手术中植入了 220 个 DE(中位数长度为 49.3mm,范围 25.1-93.8)(范围 3-16 个/手术)。除一个植入的 DE 外(99.5%),所有植入的 DE 术后均检测到足够的 SEEG 信号;在 17 名患者中有 15 名(88.2%)确定了 EZ,8 名患者(47.1%)最终进行了焦点切除。平均偏差为 EP 为 3.2±2.4mm,CP 为 3.0±2.2mm,TP 为 2.7±2.0mm。一名患者发生术后 SEEG 相关发病率(即保守治疗的迟发性细菌性脑膜炎)。未记录到死亡或新的神经功能缺损。
VG-SEEG 的准确性足以确定 DRE 患者的 EZ,且风险状况良好。它是一种可行且安全的框架或机器人系统替代方案。