Gwak Dong-Seok, Hwang Yang-Ha, Kim Yong-Won
Department of Neurology, School of Medicine, Kyungpook National University, Daegu, South Korea.
Department of Neurology, Kyungpook National University Hospital, Daegu, South Korea.
Front Neurol. 2021 Jan 29;11:617142. doi: 10.3389/fneur.2020.617142. eCollection 2020.
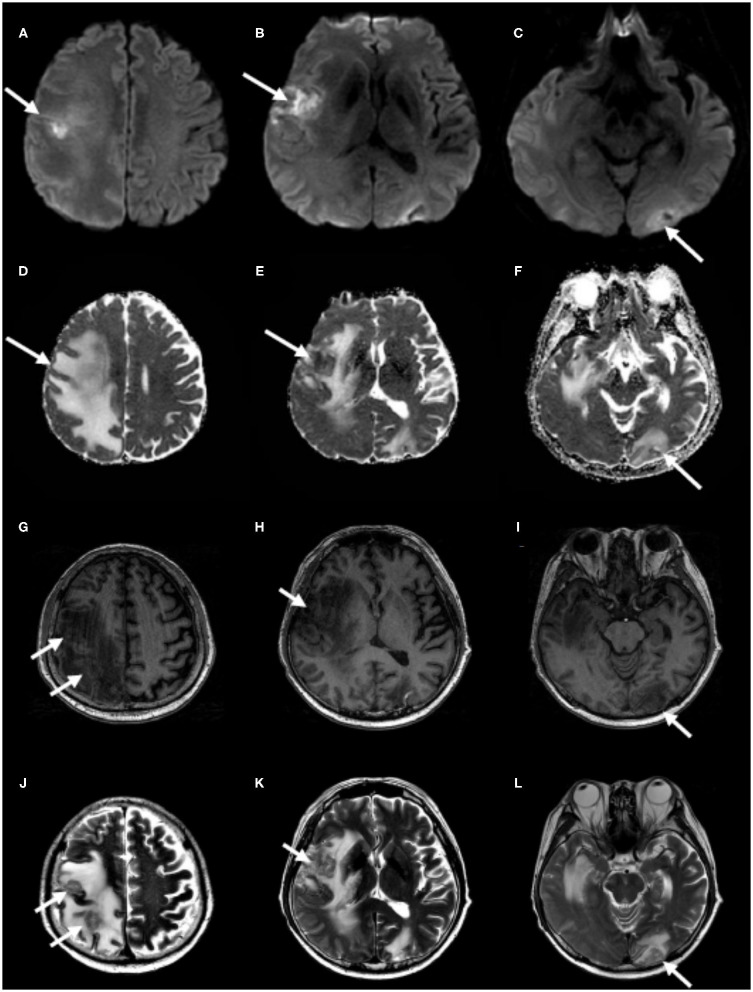
Ischemic stroke and cancer are frequent in the elderly and are the two common causes of death and disability. They are related to each other, and cancer may lead to ischemic stroke and vice versa. If patients with cancer exhibited recurrent acute neurological deficits after index stroke, a cancer-related stroke could be considered. However, a brain metastasis is another common cause of neurological complications and has a poor prognosis in patients with ischemic stroke and comorbid cancer. Here, we report a rare case of metastatic cancer that occurred after index stroke in a patient with renal cell carcinoma (RCC) and unusual imaging findings. Through the case, we discuss the pathophysiology and probable predisposing factors for metastatic disease in areas of infarction. A 48-year-old man presented with sudden onset of left facial palsy and hemiparesis. He had a history of hypertension and RCC with pulmonary metastases treated with radical nephrectomy and chemotherapy. Brain magnetic resonance imaging (MRI) revealed multiple scattered acute infarctions in the right insular, frontal, parietal, and left occipital cortices. There were no definite sources of embolism. Eight months after the index stroke, he presented with subacute onset of progressive left hemiparesis. He had no focal neurological deficits except left-sided weakness and left nasolabial fold blunting. MRI scan demonstrated partial diffusion restriction on the right frontotemporal cortices without decline of apparent diffusion coefficient values on the corresponding lesions and T1 hypointensities and T2 hyperintensities with perilesional vasogenic edema on the right insular, frontal, parietal, and left occipital cortices, indicative of brain metastases confined to the area of previous infarctions. Cerebral infarctions can cause neovascularization and disruption of the blood-brain barrier. Moreover, the compartmentalized cavity formed by the ischemic injury may accept a large volume of metastatic tumor cells. Such an altered microenvironment of infarcted tissue would be suitable for the colonization and proliferation of metastatic seed. Further, brain metastases should be considered, in addition to recurrence, when new focal neurological deficits develop in patients with ischemic stroke and comorbid cancer.
缺血性中风和癌症在老年人中很常见,是导致死亡和残疾的两个常见原因。它们相互关联,癌症可能导致缺血性中风,反之亦然。如果癌症患者在首次中风后出现反复急性神经功能缺损,则可能考虑为癌症相关性中风。然而,脑转移瘤是神经并发症的另一个常见原因,在合并癌症的缺血性中风患者中预后较差。在此,我们报告一例罕见的转移性癌症病例,该病例发生在一名肾细胞癌(RCC)患者的首次中风后,且具有不寻常的影像学表现。通过该病例,我们讨论了梗死区域转移性疾病的病理生理学和可能的诱发因素。一名48岁男性突发左侧面瘫和偏瘫。他有高血压病史,曾患肾细胞癌伴肺转移,接受过根治性肾切除术和化疗。脑部磁共振成像(MRI)显示右侧岛叶、额叶、顶叶和左侧枕叶皮质有多个散在的急性梗死灶。没有明确的栓塞来源。首次中风8个月后,他出现渐进性左侧偏瘫亚急性发作。除左侧无力和左侧鼻唇沟变浅外,他没有局灶性神经功能缺损。MRI扫描显示右侧额颞叶皮质有部分扩散受限,相应病变的表观扩散系数值无下降,右侧岛叶、额叶、顶叶和左侧枕叶皮质有T1低信号和T2高信号,并伴有病灶周围血管源性水肿,提示脑转移瘤局限于先前梗死区域。脑梗死可导致新生血管形成和血脑屏障破坏。此外,缺血性损伤形成的分隔腔可能容纳大量转移性肿瘤细胞。梗死组织这种改变的微环境将适合转移性种子的定植和增殖。此外,对于合并癌症的缺血性中风患者,当出现新的局灶性神经功能缺损时,除了复发外,还应考虑脑转移瘤。