Arnanz Ana, De Munck Neelke, El Khatib Ibrahim, Bayram Aşina, Abdala Andrea, Melado Laura, Lawrenz Barbara, Coughlan Carol, Pacheco Alberto, Garcia-Velasco Juan A, Fatemi Human M
ART Fertility Clinic, Abu Dhabi/Dubai, United Arab Emirates.
Obstetrical Department, Women's University Hospital Tuebingen, Tuebingen, Germany.
Front Endocrinol (Lausanne). 2021 Jan 25;11:609524. doi: 10.3389/fendo.2020.609524. eCollection 2020.
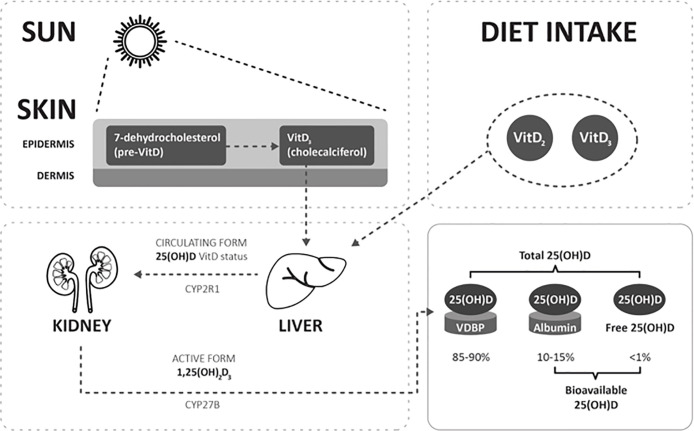
The widespread distribution of the Vitamin D (VitD) receptor in reproductive tissues suggests an important role for VitD in human reproduction. The assessment of patient´s VitD is based on the 25-hydroxyvitamin D (25(OH)D) metabolite measurement. However, most of the circulating 25(OH)D is bound to either VitD-binding protein (VDBP) (88%) or albumin (12%) and less than 1% circulates free.
To determine a possible correlation between VitD levels in serum (S) and follicular fluid (FF) and blastocyst ploidy status in patients undergoing infertility treatment.
A prospective observational study was performed including couples planned for preimplantation genetic testing for aneuploidies (PGT-A) from ART Fertility Clinics. Patients were classified according to their 25(OH)D-Serum levels: VitD deficient group <20 ng/ml and insufficient/replete ≥20 ng/ml defined as VitD non-deficient group.
Serum samples and 226 FF from individual follicles were collected for 25(OH)D, bioavailable 25(OH)D, free 25(OH)D, and % free 25(OH)D measurement. 25(OH)D-Serum in VitD deficient and non-deficient were 13.2±4.0 ng/ml vs 32.3±9.2 ng/ml; p<0.001. FF from 40 and 74 biopsied blastocysts was analysed of which 52.5 and 60.8% were euploid (p = 0.428), respectively. In VitD deficient patients, mean 25(OH)D-FF, bioavailable 25(OH)D-FF, and free 25(OH)D-FF were higher in euploid vs aneuploid blastocysts (18.3±6.3 ng/ml vs 13.9±4.8 ng/ml; p = 0.040; 1.5±0.5 ng/ml vs 1.1±0.4 ng/ml; p = 0.015; 0.005±0.002 ng/ml vs 0.003±0.001 ng/ml; p = 0.023, respectively), whilst no differences were found in VitD non-deficient patients (37.9±12.3 ng/ml vs 40.6±13.7 ng/ml; p = 0.380; 3.1±1.1 ng/ml vs 3.3±1.2 ng/ml; p = 0.323; 0.01±0.003 ng/ml vs 0.01±0.004 ng/ml; p = 0.319, respectively).
VitD non-deficient patients have a significantly higher probability of obtaining a euploid blastocyst compared to VitD deficient patients (OR:33.36, p = 0.002).
维生素D(VitD)受体在生殖组织中的广泛分布表明VitD在人类生殖中具有重要作用。对患者VitD的评估基于25-羟基维生素D(25(OH)D)代谢物的测量。然而,大多数循环中的25(OH)D与VitD结合蛋白(VDBP)(88%)或白蛋白(12%)结合,游离循环的不到1%。
确定接受不孕症治疗患者的血清(S)和卵泡液(FF)中VitD水平与囊胚倍性状态之间可能存在的相关性。
进行了一项前瞻性观察研究,纳入了来自辅助生殖技术生育诊所计划进行非整倍体植入前基因检测(PGT-A)的夫妇。患者根据其25(OH)D血清水平进行分类:VitD缺乏组<20 ng/ml,不足/充足组≥20 ng/ml定义为VitD非缺乏组。
收集了血清样本和来自单个卵泡的226份FF,用于测量25(OH)D、生物可利用的25(OH)D、游离25(OH)D和游离25(OH)D百分比。VitD缺乏组和非缺乏组的25(OH)D血清分别为13.2±4.0 ng/ml和32.3±9.2 ng/ml;p<0.001。对40个和74个活检囊胚的FF进行了分析,其中分别有52.5%和60.8%为整倍体(p = 0.428)。在VitD缺乏的患者中,整倍体囊胚的平均25(OH)D-FF、生物可利用的25(OH)D-FF和游离25(OH)D-FF高于非整倍体囊胚(18.3±6.3 ng/ml对13.9±4.8 ng/ml;p = 0.040;1.5±0.5 ng/ml对1.1±0.4 ng/ml;p = 0.015;0.005±0.002 ng/ml对0.003±0.001 ng/ml;p = 0.023),而在VitD非缺乏的患者中未发现差异(37.9±12.3 ng/ml对40.6±13.7 ng/ml;p = 0.380;3.1±1.1 ng/ml对3.3±1.2 ng/ml;p = 0.323;0.