Division of Nephrology, San Francisco/ San Francisco General Hospital Renal Center, University of California, Box 1341, 1001 Potrero Avenue, Bldg 100, Room 342, San Francisco, CA, 94110, USA.
Department of Medicine, Johns Hopkins School of Medicine, Baltimore, MD, USA.
BMC Nephrol. 2021 Feb 16;22(1):60. doi: 10.1186/s12882-021-02264-7.
While catheters are often thought the result of emergency hemodialysis (HD) initiation among patients with little or no pre-dialysis nephrology care, the role of patient level of engagement in care and modality decision-making have not been fully explored.
This is a retrospective medical record review of adults (age 18-89 years) who received care in academically affiliated private practice, public hospital, or Veterans Administration settings prior to initiating HD with a catheter between 10/1/2011 and 9/30/2012. Primary predictors were level of patient engagement in nephrology care within 6 months of HD initiation and timing of modality decision-making. Primary outcomes were provider action (referral) and any patient action (evaluation by a vascular surgeon, vein mapping or vascular surgery) toward [arteriovenous fistula or graft, (AVF/AVG)] creation.
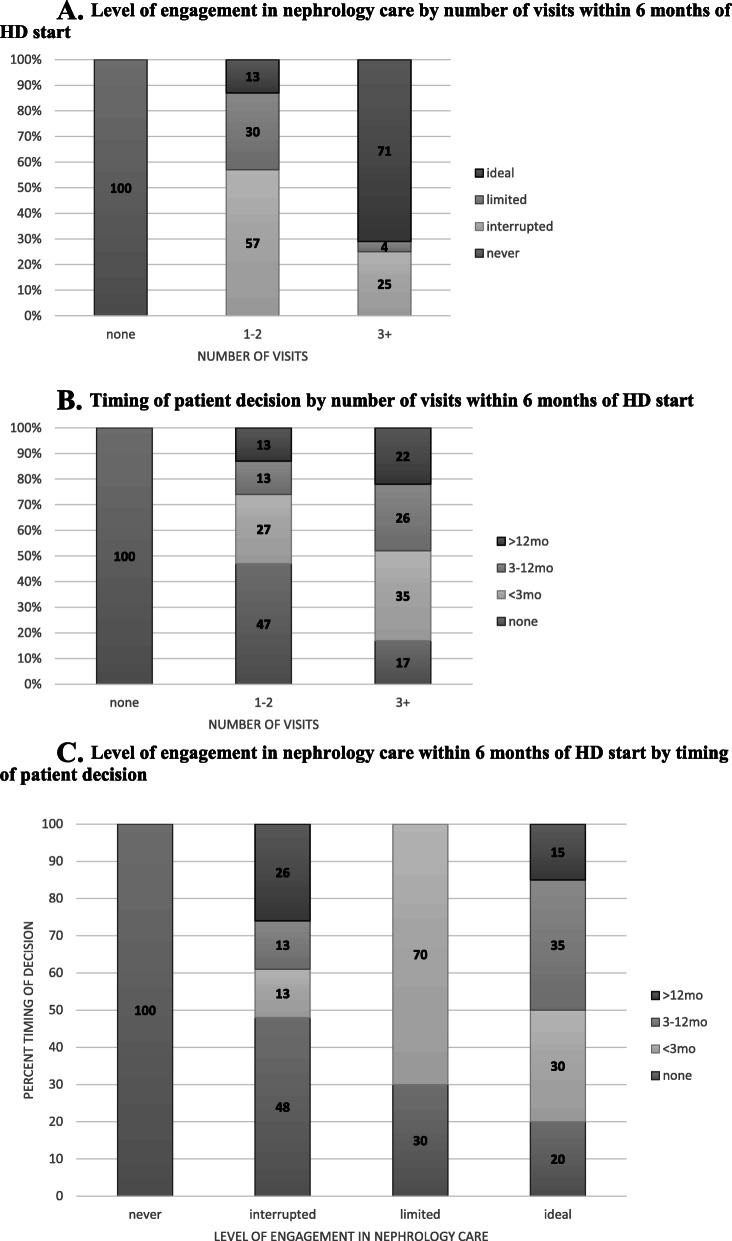
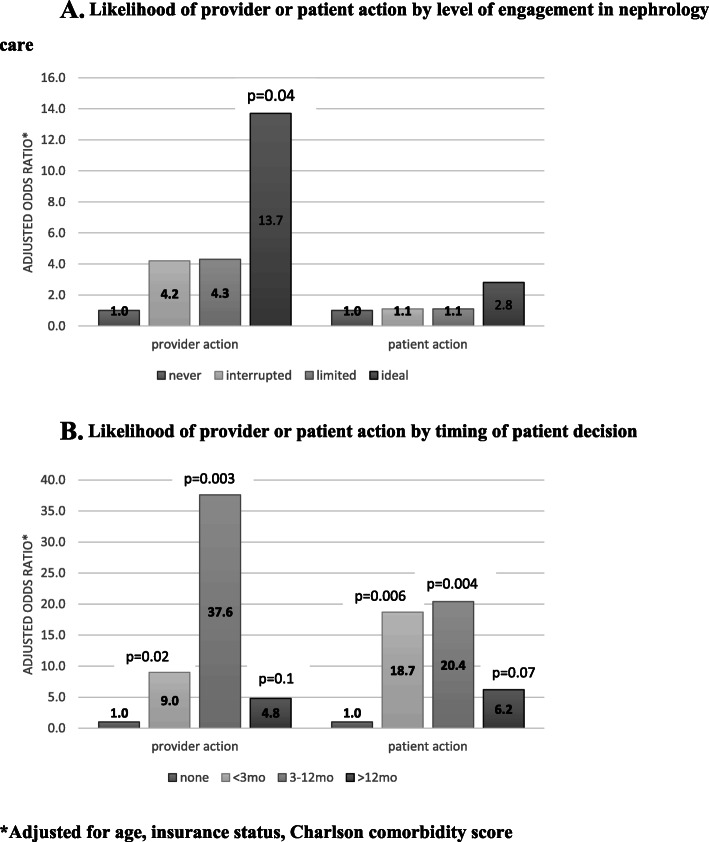
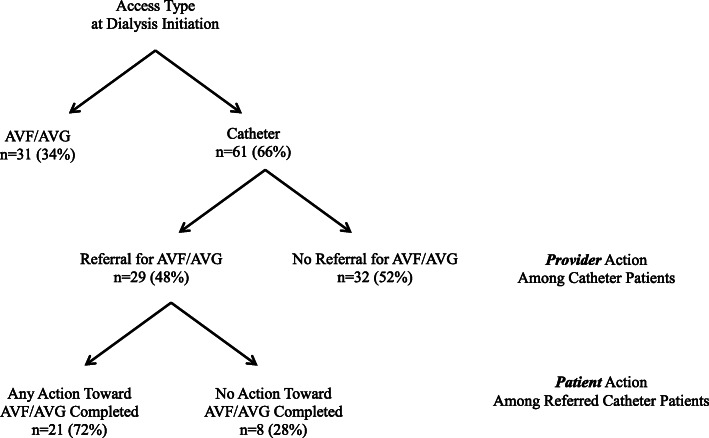
Among 92 incident HD patients, 66% (n = 61) initiated HD via catheter, of whom 34% (n = 21) had ideal engagement in care but 42% (n = 25) had no documented decision. Providers referred 48% (n = 29) of patients for AVF/AVG, of whom 72% (n = 21) took any action. Ideal engagement in care predicted provider action (adjusted OR 13.7 [95% CI 1.08, 175.1], p = 0.04), but no level of engagement in care predicted patient action (p > 0.3). Compared to patients with no documented decision, those with documented decisions within 3, 3-12, or more than 12 months before initiating dialysis were more likely to have provider action toward AVF/AVG (adjusted OR [95% CI]: 9.0 [1.4,55.6], p = 0.2, 37.6 [3.3423.4] p = 0.003, and 4.8 [0.8, 30.6], p = 0.1, respectively); and patient action (adjusted OR [95% CI]: 18.7 [2.3, 149.0], p = 0.006, 20.4 [2.6, 160.0], p = 0.004, and 6.2 [0.9, 44.0], p = 0.07, respectively).
Timing of patient modality decision-making, but not level of engagement in pre-dialysis nephrology care, was predictive of patient and provider action toward AVF/AVG Interventions addressing patients' psychological preparation for dialysis are needed.
尽管导管通常被认为是接受紧急血液透析(HD)治疗的患者在接受透析前很少或没有接受肾脏科护理的结果,但患者参与护理的程度和治疗方式决策的作用尚未得到充分探讨。
这是一项回顾性病历审查,纳入了 2011 年 10 月 1 日至 2012 年 9 月 30 日期间在学术附属私人诊所、公立医院或退伍军人管理局接受 HD 治疗并伴有导管的成年患者(年龄 18-89 岁)。主要预测因素为 HD 治疗前 6 个月内患者参与肾脏科护理的程度和治疗方式决策的时间。主要结果为提供者的行动(转诊)和任何患者的行动(血管外科医生评估、静脉图或血管手术),以建立动静脉瘘或移植物(AVF/AVG)。
在 92 例新发生的 HD 患者中,66%(n=61)通过导管开始 HD 治疗,其中 34%(n=21)患者的护理参与度理想,但 42%(n=25)患者无记录的决策。提供者为 48%(n=29)的患者转诊 AVF/AVG,其中 72%(n=21)采取了任何行动。理想的护理参与度预测了提供者的行动(调整后的 OR 13.7 [95%CI 1.08,175.1],p=0.04),但没有任何参与度水平预测患者的行动(p>0.3)。与无记录决策的患者相比,在开始透析前 3 个月、3-12 个月或 12 个月以上有记录决策的患者更有可能采取提供者的行动(调整后的 OR [95%CI]:9.0 [1.4,55.6],p=0.2,37.6 [3.3423.4],p=0.003,4.8 [0.8,30.6],p=0.1),并且患者也更有可能采取行动(调整后的 OR [95%CI]:18.7 [2.3,149.0],p=0.006,20.4 [2.6,160.0],p=0.004,6.2 [0.9,44.0],p=0.07)。
患者治疗方式决策的时间,而不是接受透析前肾脏科护理的程度,是预测患者和提供者采取 AVF/AVG 干预措施的重要因素。需要针对患者的心理准备进行干预,以促进患者接受透析治疗。