Department of Health Services, Policy and Practice, Brown University School of Public Health, Providence, Rhode Island.
Center for Gerontology and Healthcare Research, Brown University School of Public Health, Providence, Rhode Island.
JAMA Netw Open. 2021 Feb 1;4(2):e2037320. doi: 10.1001/jamanetworkopen.2020.37320.
The Hospital Readmissions Reduction Program publicly reports and financially penalizes hospitals according to 30-day risk-standardized readmission rates (RSRRs) exclusively among traditional Medicare (TM) beneficiaries but not persons with Medicare Advantage (MA) coverage. Exclusively reporting readmission rates for the TM population may not accurately reflect hospitals' readmission rates for older adults.
To examine how inclusion of MA patients in hospitals' performance is associated with readmission measures and eligibility for financial penalties.
DESIGN, SETTING, AND PARTICIPANTS: This is a retrospective cohort study linking the Medicare Provider Analysis and Review file with the Healthcare Effectiveness Data and Information Set at 4070 US acute care hospitals admitting both TM and MA patients. Participants included patients admitted and discharged alive with a diagnosis of acute myocardial infarction (AMI), congestive heart failure (CHF), or pneumonia between 2011 and 2015. Data analyses were conducted between April 1, 2018, and November 20, 2020.
Admission to an acute care hospital.
The outcome was readmission for any reason occurring within 30 days after discharge. Each hospital's 30-day RSRR was computed on the basis of TM, MA, and all patients and estimated changes in hospitals' performance and eligibility for financial penalties after including MA beneficiaries for calculating 30-day RSRRs.
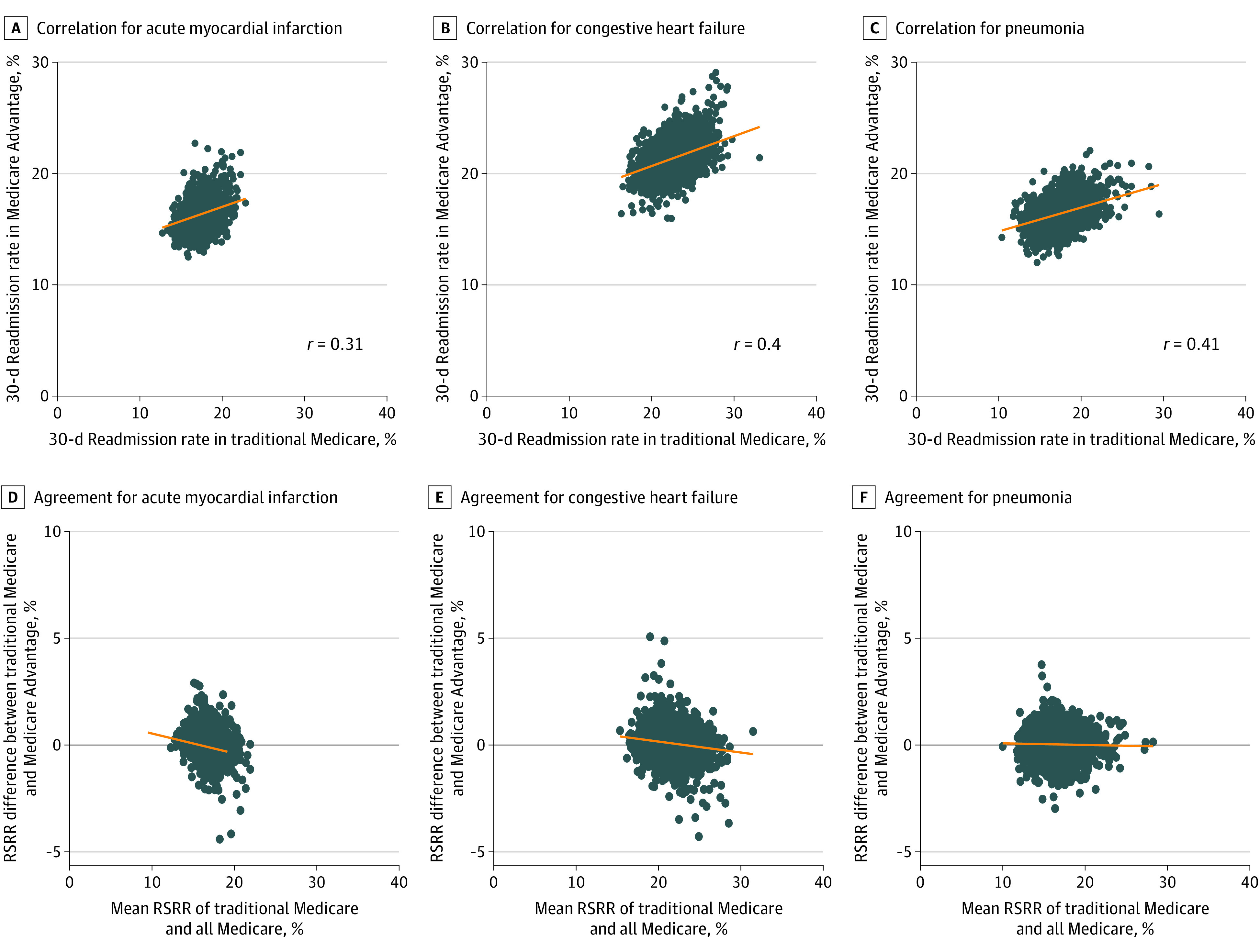
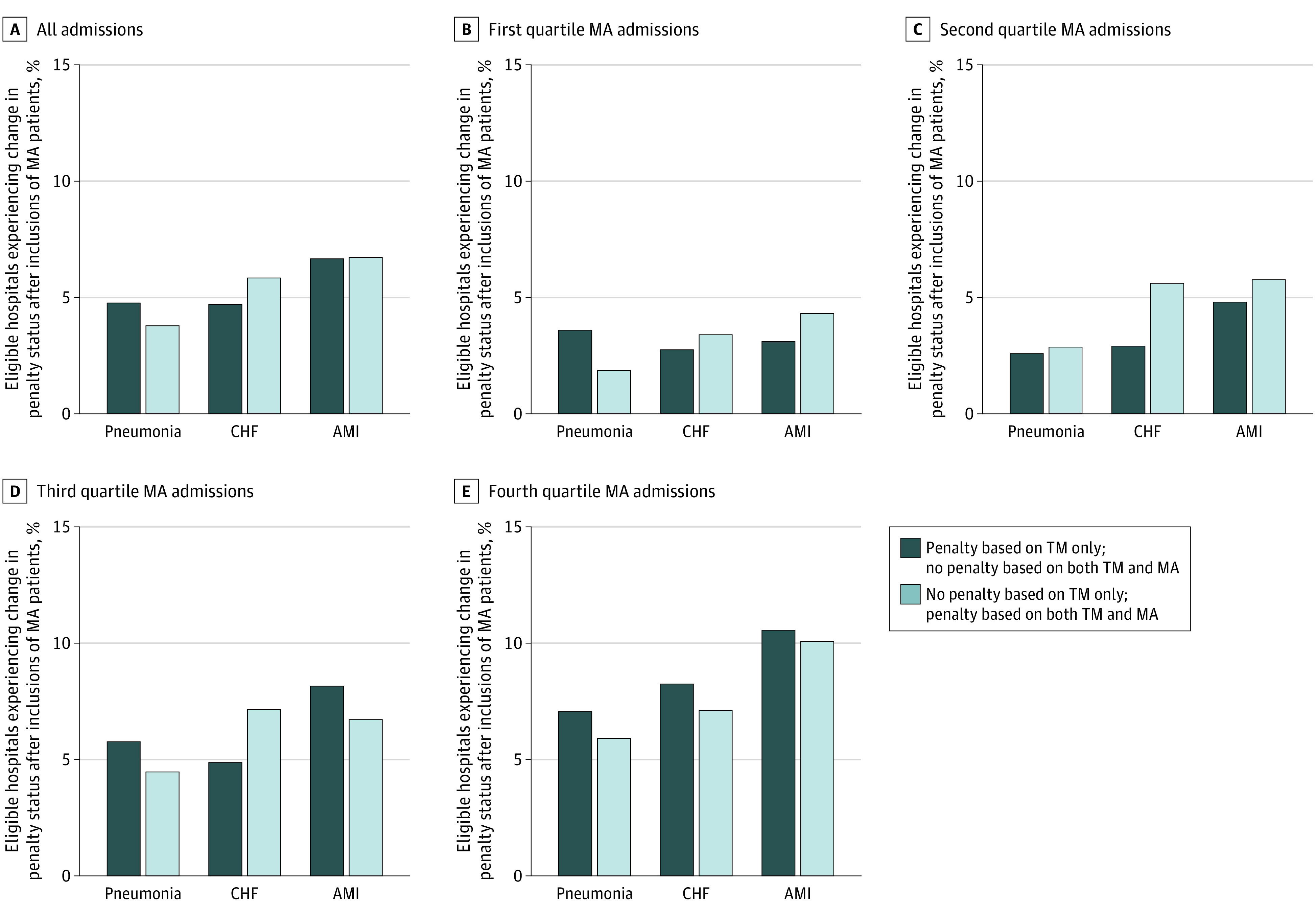
There were 748 033 TM patients (mean [SD] age, 76.8 [83] years; 360 692 [48.2%] women) and 295 928 MA patients (mean [SD] age, 77.5 [7.9] years; 137 422 [46.4%] women) hospitalized and discharged alive for AMI; 1 327 551 TM patients (mean [SD] age, 81 [8.3] years; 735 855 [55.4%] women) and 457 341 MA patients (mean [SD] age, 79.8 [8.1] years; 243 503 [53.2%] women) for CHF; and 2 017 020 TM patients (mean [SD] age, 80.7 [8.5] years; 1 097 151 [54.4%] women) and 610 790 MA patients (mean [SD] age, 79.6 [8.2] years; 321 350 [52.6%] women) for pneumonia. The 30-day RSRRs for TM and MA patients were correlated (correlation coefficients, 0.31 for AMI, 0.40 for CHF, and 0.41 for pneumonia) and the TM-based RSRR systematically underestimated the RSRR for all Medicare patients for each condition. Of the 2820 hospitals with 25 or more admissions for at least 1 of the outcomes of AMI, CHF, and pneumonia, 635 (23%) had a change in their penalty status for at least 1 of these conditions after including MA data. Changes in hospital performance and penalty status with the inclusion of MA patients were greater for hospitals in the highest quartile of MA admissions.
In this cohort study, the inclusion of data from MA patients changed the penalty status of a substantial fraction of US hospitals for at least 1 of 3 reported conditions. This suggests that policy makers should consider including all hospital patients, regardless of insurance status, when assessing hospital quality measures.
重要性:医院再入院率降低计划根据 30 天风险标准化再入院率(RSRR)专门向传统医疗保险(TM)受益人和医疗保险优势(MA)覆盖的人群报告和经济处罚医院,但不包括 MA 患者。仅报告 TM 人群的再入院率可能无法准确反映医院对老年人的再入院率。
目的:研究将 MA 患者纳入医院绩效与再入院措施和经济处罚资格的关系。
设计、地点和参与者:这是一项回顾性队列研究,将医疗保险提供者分析和审查文件与医疗保健效果数据和信息集在 4070 家美国急性护理医院进行链接,这些医院同时收治 TM 和 MA 患者。参与者包括 2011 年至 2015 年期间因急性心肌梗死(AMI)、充血性心力衰竭(CHF)或肺炎住院并存活出院的患者。数据分析于 2018 年 4 月 1 日至 2020 年 11 月 20 日进行。
暴露:入住急性护理医院。
主要结果和测量:结果是出院后 30 天内任何原因的再入院。根据 TM、MA 和所有患者计算每家医院的 30 天 RSRR,并估计在包括 MA 受益人计算 30 天 RSRR 后,医院绩效和经济处罚资格的变化。
结果:有 748033 名 TM 患者(平均[标准差]年龄,76.8[83]岁;360692[48.2%]女性)和 295928 名 MA 患者(平均[标准差]年龄,77.5[7.9]岁;137422[46.4%]女性)因 AMI 住院并存活出院;1327551 名 TM 患者(平均[标准差]年龄,81[8.3]岁;735855[55.4%]女性)和 457341 名 MA 患者(平均[标准差]年龄,79.8[8.1]岁;243503[53.2%]女性)因 CHF 住院并存活出院;2017020 名 TM 患者(平均[标准差]年龄,80.7[8.5]岁;1097151[54.4%]女性)和 610790 名 MA 患者(平均[标准差]年龄,79.6[8.2]岁;321350[52.6%]女性)因肺炎住院并存活出院。TM 和 MA 患者的 30 天 RSRR 相关(相关系数,AMI 为 0.31,CHF 为 0.40,肺炎为 0.41),TM 为基础的 RSRR 系统地低估了所有 Medicare 患者的 RSRR 对于每种情况。在 2820 家至少有 25 名 AMI、CHF 和肺炎至少有 1 项结果的医院中,有 635 家(23%)在至少有 1 项条件下的处罚状态发生了变化。在包括 MA 患者数据后,医院绩效和处罚状态的变化在 MA 入院量最高的四分之一的医院中更大。
结论和相关性:在这项队列研究中,至少有 3 种报告疾病之一的美国医院的处罚状态发生了实质性变化,其中包括 MA 患者的数据。这表明政策制定者在评估医院质量措施时,应考虑将所有医院患者(无论保险状况如何)纳入其中。