Li Jingen, Somers Virend K, Gao Xiang, Chen Zhuo, Ju Jianqing, Lin Qian, Mohamed Essa A, Karim Shahid, Xu Hao, Zhang Lijing
Department of Cardiology, Dongzhimen Hospital, Beijing University of Chinese Medicine, Beijing, China.
Department of Cardiovascular Medicine, Mayo Clinic, Rochester, Minnesota.
JAMA Netw Open. 2021 Feb 1;4(2):e2037554. doi: 10.1001/jamanetworkopen.2020.37554.
Extremely low diastolic blood pressure has been reported to be associated with increased adverse cardiovascular events (ie, the diastolic J-shape phenomenon); however, current US guidelines recommend an intensive blood pressure target of less than 130/80 mm Hg without mentioning the lower limits of diastolic blood pressure.
To evaluate whether there is a diastolic J-shape phenomenon for patients with an treated systolic blood pressure of less than 130 mm Hg and to explore the safe and optimal diastolic blood pressure ranges for this patient population.
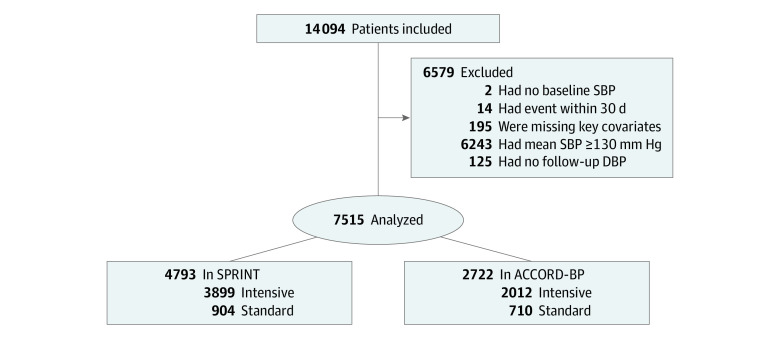
DESIGN, SETTING, AND PARTICIPANTS: This cohort study analyzed outcome data of patients at high cardiovascular risk who were randomized to intensive or standard blood pressure control and achieved treated systolic blood pressure of less than 130 mm Hg in the Systolic Blood Pressure Intervention Trial (SPRINT) and Action to Control Cardiovascular Risk in Diabetes-Blood Pressure (ACCORD-BP) trial. Data were collected from October 2010 to August 2015 (SPRINT) and from September 1999 to June 2009 (ACCORD-BP). Data were analyzed from January to May 2020.
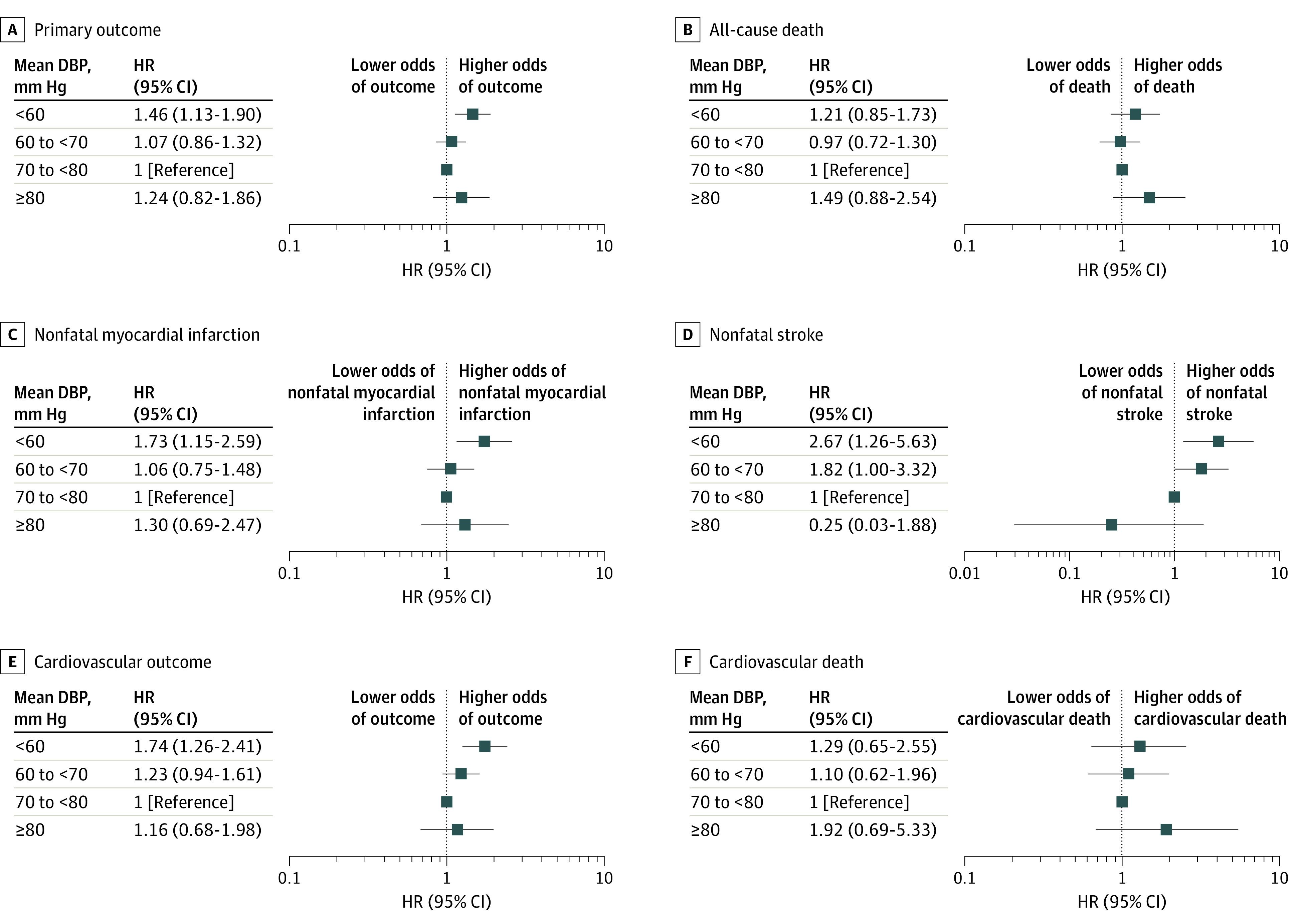
Treated diastolic blood pressure, divided in intervals of less than 60, 60 to less than 70, 70 to less than 80, and 80 mm Hg and greater.
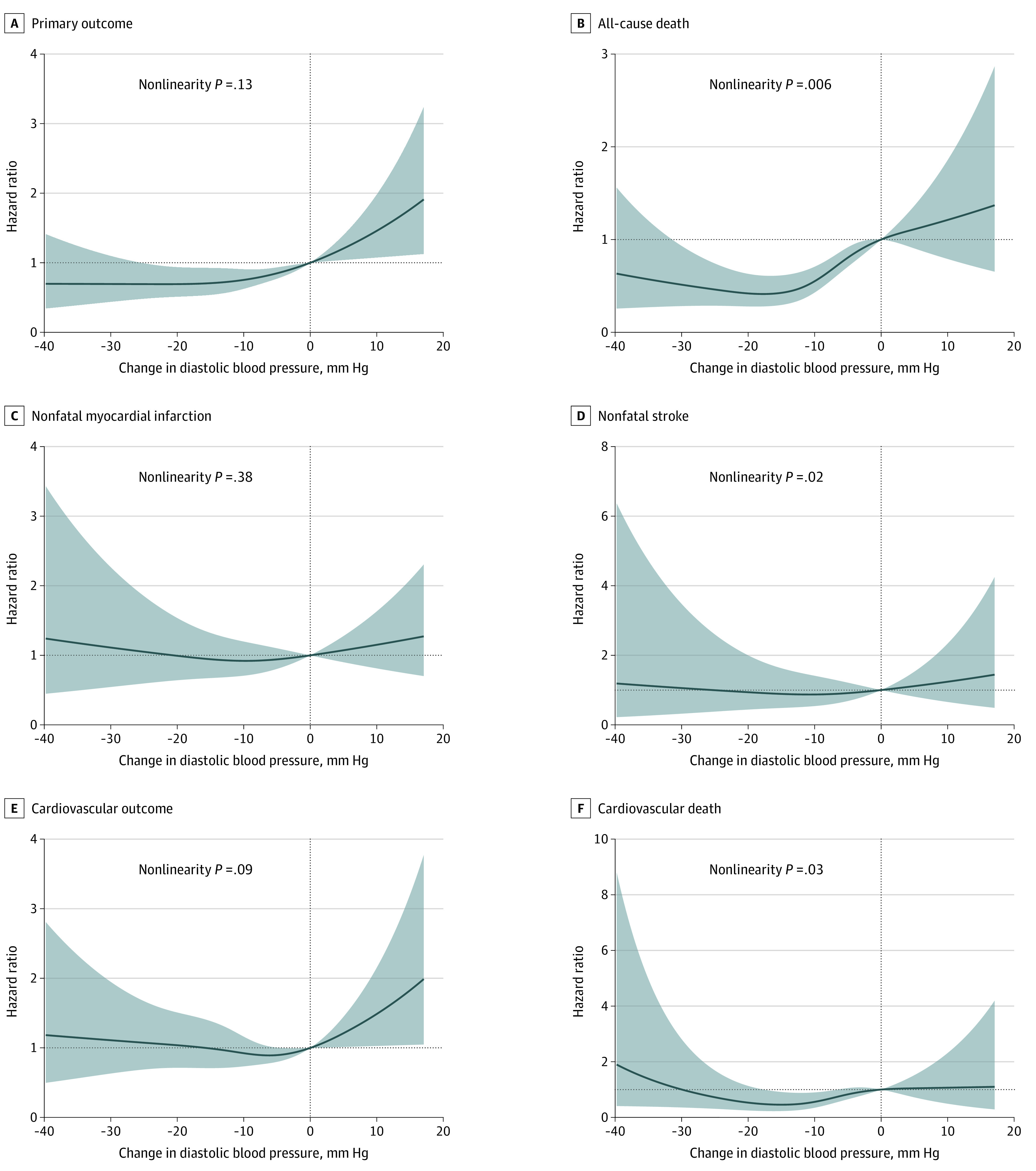
The primary outcome was a composite of all-cause death, nonfatal myocardial infarction, and nonfatal stroke. A composite cardiovascular outcome, including cardiovascular death, nonfatal myocardial infarction, and nonfatal stroke, was among the key secondary outcomes.
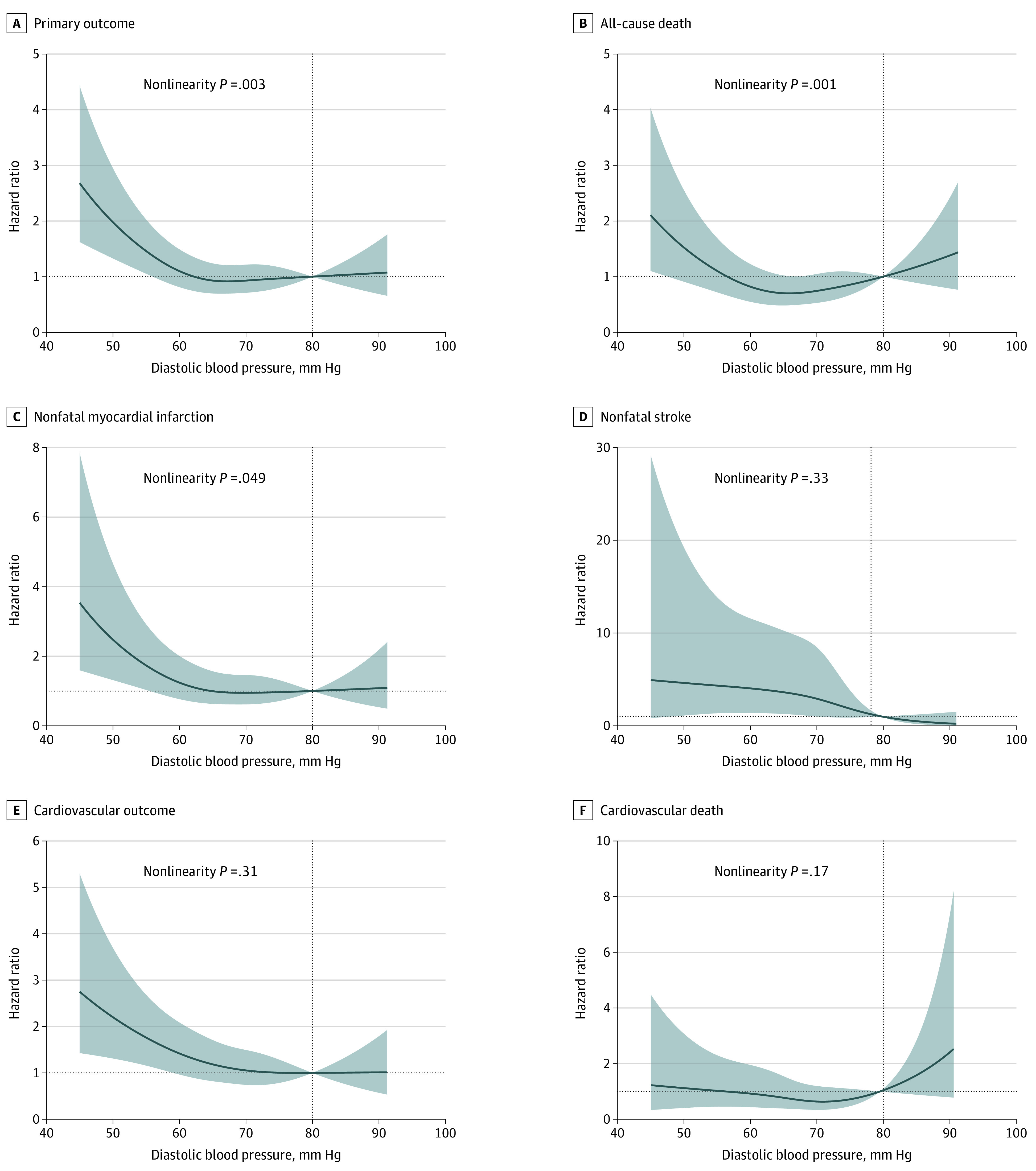
A total of 7515 patients (mean [SD] age, 65.6 [8.7] years; 4553 [60.6%] men) were included in this analysis. The nominally lowest risk was observed at a diastolic blood pressure between 70 and 80 mm Hg for the primary outcome, the composite cardiovascular outcome, nonfatal myocardial infarction, and cardiovascular death. A mean diastolic blood pressure of less than 60 mm Hg was associated with significantly increased risk of the primary outcome (hazard ratio [HR], 1.46; 95% CI, 1.13-1.90; P = .004), the composite cardiovascular outcome (HR, 1.74; 95% CI, 1.26-2.41; P = .001), nonfatal myocardial infarction (HR, 1.73; 95% CI, 1.15-2.59; P = .008), and nonfatal stroke (HR, 2.67; 95% CI, 1.26-5.63; P = .01).
This cohort study found that lowering diastolic blood pressure to less than 60 mm Hg was associated with increased risk of cardiovascular events in patients with high cardiovascular risk and an treated systolic blood pressure less than 130 mm Hg. The finding that a diastolic blood pressure value between 70 and 80 mm Hg was an optimum target for this patient population merits further study.
据报道,极低的舒张压与不良心血管事件增加相关(即舒张期J形现象);然而,美国当前的指南推荐强化血压目标为低于130/80 mmHg,却未提及舒张压的下限。
评估收缩压治疗后低于130 mmHg的患者是否存在舒张期J形现象,并探索该患者群体安全且最佳的舒张压范围。
设计、设置和参与者:这项队列研究分析了心血管疾病高风险患者的结局数据,这些患者在收缩压干预试验(SPRINT)和糖尿病血压控制行动(ACCORD-BP)试验中被随机分配至强化或标准血压控制组,且收缩压治疗后低于130 mmHg。数据收集于2010年10月至2015年8月(SPRINT)以及1999年9月至2009年6月(ACCORD-BP)。数据分析于2020年1月至5月进行。
治疗后的舒张压,分为低于60 mmHg、60至低于70 mmHg、70至低于80 mmHg以及80 mmHg及以上几个区间。
主要结局为全因死亡、非致死性心肌梗死和非致死性卒中的复合结局。包括心血管死亡、非致死性心肌梗死和非致死性卒中的复合心血管结局是关键次要结局之一。
本分析共纳入7515例患者(平均[标准差]年龄为65.6[8.7]岁;4553例[60.6%]为男性)。对于主要结局、复合心血管结局、非致死性心肌梗死和心血管死亡,在舒张压为70至80 mmHg时观察到名义上最低的风险。平均舒张压低于60 mmHg与主要结局风险显著增加相关(风险比[HR],1.46;95%置信区间[CI],1.13 - 1.90;P = 0.004)、复合心血管结局(HR,1.74;95% CI,1.26 - 2.41;P = 0.001)、非致死性心肌梗死(HR,1.73;95% CI,1.15 - 2.59;P = 0.008)以及非致死性卒中(HR,2.67;95% CI,1.26 - 5.63;P = 0.01)。
这项队列研究发现,将心血管疾病高风险且收缩压治疗后低于130 mmHg的患者的舒张压降至低于60 mmHg与心血管事件风险增加相关。舒张压值在70至80 mmHg之间是该患者群体的最佳目标这一发现值得进一步研究。