Morinaga Hiroaki, Kato Ken, Hisagi Motoyuki, Tanaka Hiroyuki
Department of Cardiology, Tokyo Metropolitan Tama Medical Center, Tokyo, Japan.
Department of Cardiovascular Surgery, Tokyo Metropolitan Tama Medical Center, Tokyo, Japan.
Eur Heart J Case Rep. 2020 Dec 29;5(2):ytaa528. doi: 10.1093/ehjcr/ytaa528. eCollection 2021 Feb.
Purulent pericarditis, a rare disease with a high associated mortality rate in patients without adequate treatment, can cause serious complications, such as perforation of the surrounding tissue and organs. is a very rare cause of purulent pericarditis.
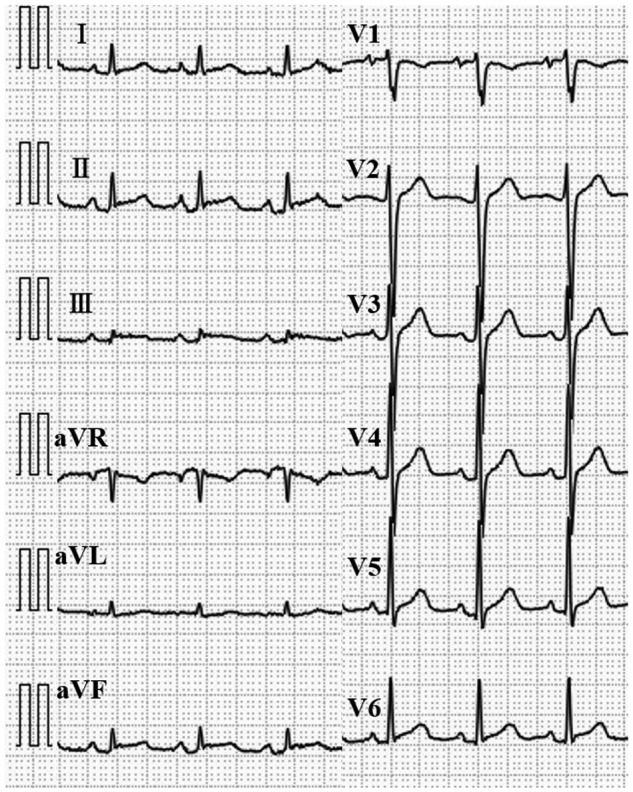
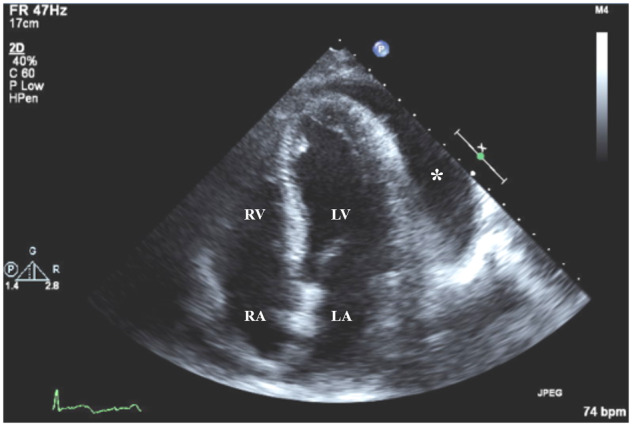
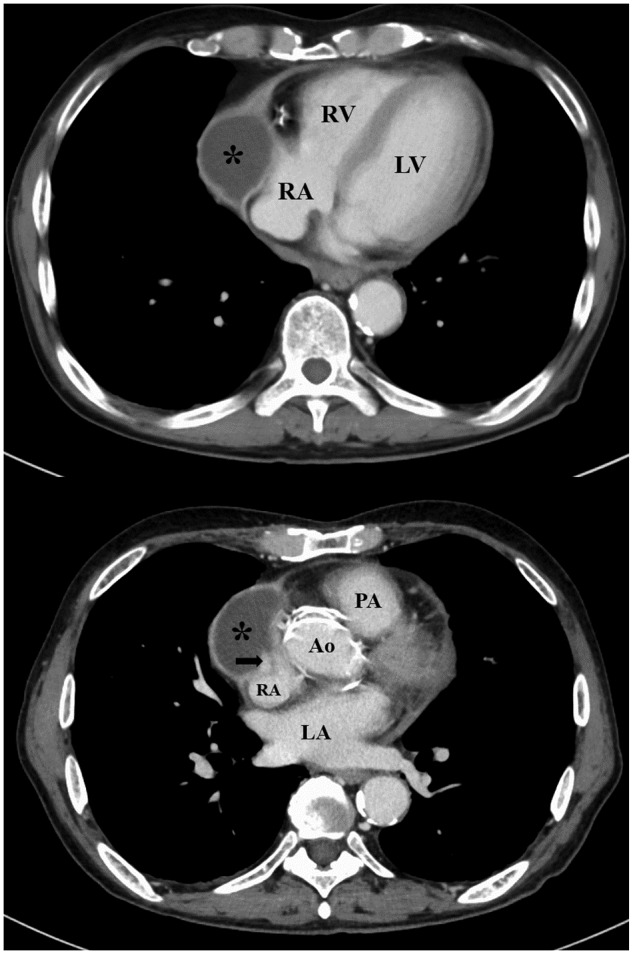
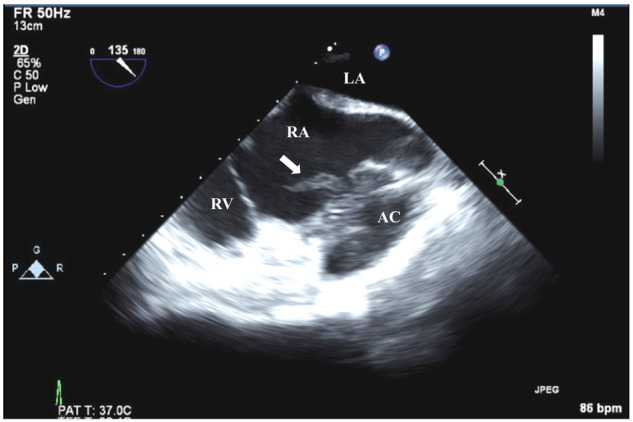
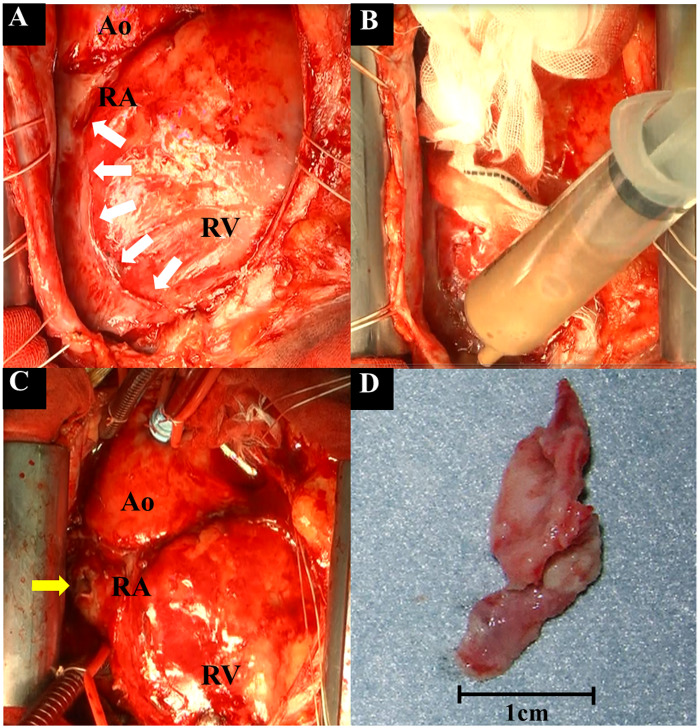
A 70-year-old male patient presented to our emergency room with chest pain of 10 days' duration. An electrocardiogram showed ST-segment elevation and PR-segment depression on multiple leads. A transthoracic echocardiogram showed normal left ventricular function and a large amount of pericardial effusion. Acute pericarditis was diagnosed, and anti-inflammatory drug therapy was initiated. Due to the lack of improvement in the symptoms, pericardiocentesis was performed on Day 8 and revealed about 800 cc of the bloody fluid. was detected in a culture of the pericardial effusion and blood. Although intravenous antibiotic therapy was initiated for purulent pericarditis, his fever persisted. Computed tomography of the chest performed on Day 14 showed an abscess cavity in the pericardial space around the right atrium (RA). Furthermore, transoesophageal echocardiography revealed vegetation in the RA. Emergency surgery confirmed the presence of vegetation and minor perforation of the RA with communication to the abscess cavity. After surgical therapy, the patient clinically improved and was discharged on Day 51.
In cases of acute pericarditis, purulent pericarditis should be considered if clinical improvement is not observed after initial treatment with anti-inflammatory drugs. Once the diagnosis of purulent pericarditis is made, aggressive source control is necessary for improved clinical outcomes.
化脓性心包炎是一种罕见疾病,在未得到充分治疗的患者中死亡率很高,可导致严重并发症,如周围组织和器官穿孔。是化脓性心包炎的一种非常罕见的病因。
一名70岁男性患者因持续10天的胸痛前来我院急诊室就诊。心电图显示多个导联ST段抬高和PR段压低。经胸超声心动图显示左心室功能正常,大量心包积液。诊断为急性心包炎,并开始抗炎药物治疗。由于症状无改善,在第8天进行了心包穿刺,抽出约800毫升血性液体。在心包积液和血液培养中检测到。尽管开始了针对化脓性心包炎的静脉抗生素治疗,但患者仍持续发热。第14天进行的胸部计算机断层扫描显示右心房(RA)周围心包腔内有脓肿腔。此外,经食管超声心动图显示RA内有赘生物。急诊手术证实存在赘生物以及RA有微小穿孔并与脓肿腔相通。手术治疗后,患者临床症状改善,于第51天出院。
在急性心包炎病例中,如果最初用抗炎药物治疗后未观察到临床改善,则应考虑化脓性心包炎。一旦确诊为化脓性心包炎,积极控制感染源对于改善临床结局是必要的。