Christopher Karen L, Patnaik Jennifer L, Ifantides Cristos, Miller D Claire, Davidson Richard S, Taravella Michael J, Lynch Anne, Wagner Brandie
University of Colorado Anschutz Medical Campus, Department of Ophthalmology, Aurora, CO, USA.
Colorado School of Public Health, Department of Biostatistics and Informatics, Aurora, CO, USA.
Clin Ophthalmol. 2021 Feb 11;15:531-539. doi: 10.2147/OPTH.S287573. eCollection 2021.
To evaluate the time cost of intraoperative aberrometry (IA), to compare IA prediction error to the prediction error associated with conventional formulas using preoperative calculations (PC) and evaluate when IA provides clinically relevant benefit.
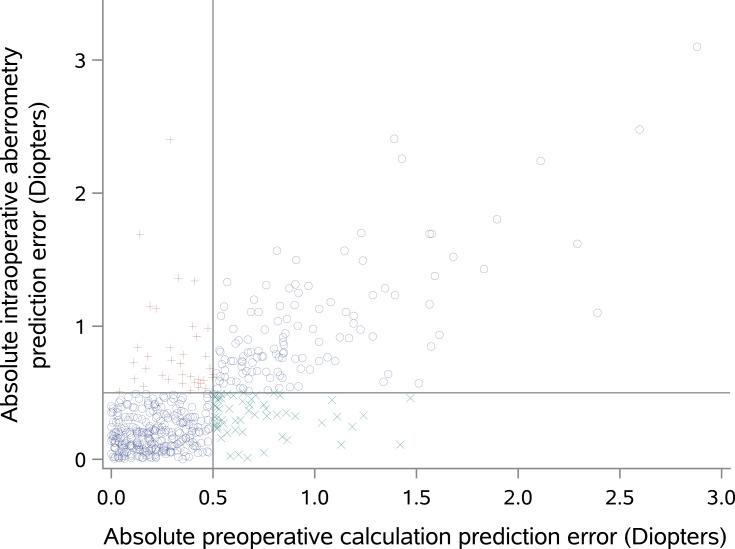
This is a retrospective study of eyes that underwent cataract phacoemulsification surgery with IA at an academic eye center. IA versus PC prediction error were compared amongst various preoperative and intraoperative characteristics. Additionally, a dichotomous variable indicating clinically relevant benefit of IA, where IA absolute prediction error was less than 0.5D and PC absolute prediction error greater than 0.5D, was associated with clinical factors.
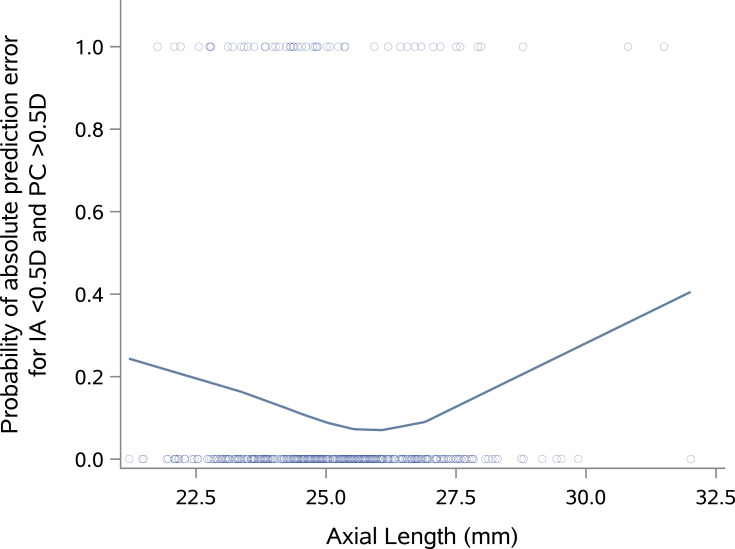
Five hundred eyes of 341 patients were included in the analysis. The quantitative difference between mean absolute prediction errors for IA versus PC was between 0.0D and 0.03D in most subgroups. For the 11.0% of eyes that had clinically relevant benefit to IA, the multivariable model identified the following strongest predictors: prior myopic corneal refractive surgery (Odds ratio (OR) 3.9, p<0.01 for myopic LASIK/PRK, OR 5.5, p=0.01 for radial keratotomy), toric or multifocal/EDOF lens implantation (OR 2.7, p=0.03 for toric monofocal lenses, OR 3.1, p=0.01 for EDOF/multifocal lenses), and short and long axial lengths (p<0.01). On average, IA implementation added 3.0 minutes to surgery (p<0.01).
For greatest likelihood of a clinically meaningful improvement in outcomes despite increased surgical time, surgeons and patients should consider using IA for eyes with extremes in axial length, eyes with prior myopic corneal refractive surgery, or when implanting lenses with toric or extended-depth-of-focus/multifocal properties.
评估术中像差仪(IA)的时间成本,将IA预测误差与使用术前计算(PC)的传统公式相关的预测误差进行比较,并评估IA何时能提供临床相关益处。
这是一项对在学术性眼科中心接受白内障超声乳化手术并使用IA的眼睛进行的回顾性研究。在各种术前和术中特征中比较IA与PC的预测误差。此外,一个二分变量表明IA的临床相关益处,即IA绝对预测误差小于0.5D且PC绝对预测误差大于0.5D,与临床因素相关。
分析纳入了341例患者的500只眼睛。在大多数亚组中,IA与PC的平均绝对预测误差之间的定量差异在0.0D至0.03D之间。对于11.0%对IA有临床相关益处的眼睛,多变量模型确定了以下最强预测因素:既往近视性角膜屈光手术(近视性准分子原位角膜磨镶术/准分子激光角膜切削术的优势比(OR)为3.9,p<0.01;放射状角膜切开术的OR为5.5,p = 0.01)、植入散光或多焦点/扩展景深(EDOF)人工晶状体(散光单焦点人工晶状体的OR为2.7,p = 0.03;EDOF/多焦点人工晶状体的OR为3.1,p = 0.01)以及短和长眼轴长度(p<0.01)。平均而言,实施IA使手术时间增加了3.0分钟(p<0.01)。
为了在手术时间增加的情况下获得临床结局有意义改善的最大可能性,外科医生和患者应考虑对眼轴长度极端的眼睛、有既往近视性角膜屈光手术史的眼睛或植入具有散光或扩展景深/多焦点特性人工晶状体的眼睛使用IA。