Gouvea Larissa, Sioufi Kareem, Brown Colin E, Waring Iv George, Chamon Wallace, Rocha Karolinne Maia
Department of Ophthalmology and Visual Sciences, University of Toronto, Toronto, ON, Canada.
Department of Ophthalmology and Visual Sciences, Federal University of São Paulo, São Paulo, Brazil.
Clin Ophthalmol. 2021 Oct 27;15:4305-4315. doi: 10.2147/OPTH.S334489. eCollection 2021.
To compare the refractive predictability of intraoperative aberrometry (IA, ORA, Alcon) and Barrett True-K/Universal II formulas for intraocular lens (IOL) power calculations in post-corneal refractive surgery and normal eyes.
Retrospective study of normal and post-corneal refractive surgery eyes that underwent cataract surgery with IA at tertiary academic center. Preoperatively, IOL power calculations were performed using Barrett Universal II (normal eyes) or Barrett True-K (post-corneal refractive surgery eyes) formulas. Intraoperatively, aphakic IA measurements were used for IOL power calculations. Mean absolute refractive prediction error (MAE) and the percentage of eyes with prediction error within ±0.50, ±0.75 and ±1.00 D were calculated. Refractive predictability was also evaluated in short, normal, and long eyes.
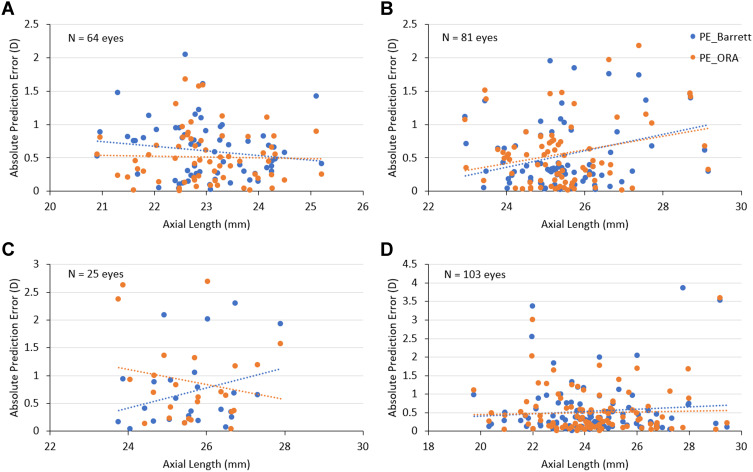
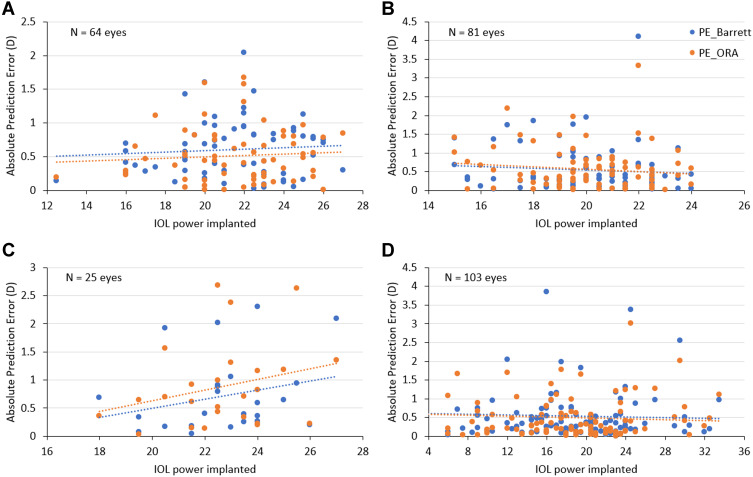
Two hundred and seventy-three eyes were included in the analysis. No statistically significant differences were observed between the MAE of preoperative formulas and IA for post-hyperopic laser vision correction (LVC), post-myopic LVC, post-radial keratotomy (RK) and normal eyes. For prediction error within ±0.5 D in post-corneal refractive surgery eyes, range of agreement between Barrett True-K and IA ranged from 28% (7/25) of the time in post-RK eyes to 49% (40/81) of the time in post-hyperopic LVC; the corresponding value for Barrett Universal II/IA was 62% (64/103) in normal eyes. When there was disagreement, IA outperformed Barrett True-K in post-hyperopic LVC eyes and Barrett formula outperformed IA in post-myopic LVC, post-RK, and normal eyes.
IA appears to be comparable to Barrett formulas for IOL power calculations in post-corneal refractive surgery and normal eyes. In post-hyperopic LVC, IA yields better results compared to Barrett True-K formula; in real-life scenarios, IA reveals statistical advantage over the Barrett True-K no history formula for eyes post-hyperopic LVC.
比较术中像差仪(IA,ORA,爱尔康)和巴雷特True-K/通用II公式在角膜屈光手术后眼和正常眼中计算人工晶状体(IOL)度数时的屈光预测性。
在三级学术中心对接受白内障手术并使用IA的正常眼和角膜屈光手术后眼进行回顾性研究。术前,使用巴雷特通用II公式(正常眼)或巴雷特True-K公式(角膜屈光手术后眼)计算IOL度数。术中,使用无晶状体IA测量值计算IOL度数。计算平均绝对屈光预测误差(MAE)以及预测误差在±0.50、±0.75和±1.00 D范围内的眼的百分比。还对短眼、正常眼和长眼的屈光预测性进行了评估。
273只眼纳入分析。在远视激光视力矫正(LVC)术后、近视LVC术后、放射状角膜切开术(RK)术后眼和正常眼中,术前公式和IA的MAE之间未观察到统计学上的显著差异。对于角膜屈光手术后眼预测误差在±0.5 D范围内的情况,巴雷特True-K与IA之间的一致范围在RK术后眼为28%(7/25),在远视LVC术后眼为49%(40/81);巴雷特通用II/IA在正常眼中的相应值为62%(64/103)。当存在差异时,IA在远视LVC术后眼中优于巴雷特True-K,而巴雷特公式在近视LVC术后眼、RK术后眼和正常眼中优于IA。
在角膜屈光手术后眼和正常眼中,IA在计算IOL度数方面似乎与巴雷特公式相当。在远视LVC术后,与巴雷特True-K公式相比,IA产生更好的结果;在实际情况中,对于远视LVC术后眼,IA相对于巴雷特True-K无历史公式具有统计学优势。