Knobel Rachel J, Ito Naoaki, Arhos Elanna K, Capin Jacob J, Buchanan Thomas S, Snyder-Mackler Lynn
University of Delaware.
Department of Physical Medicine and Rehabilitation, University of Colorado; Eastern Colorado VA Geriatric Research Education and Clinical Center.
Int J Sports Phys Ther. 2021 Feb 1;16(1):169-176. doi: 10.26603/001c.18710.
Gait asymmetries after anterior cruciate ligament reconstruction (ACLR) may lead to radiographic knee osteoarthritis. Slower walking speeds have been associated with biomarkers suggesting cartilage breakdown. The relationship between walking speed and gait symmetry after ACLR is unknown.
HYPOTHESIS/PURPOSE: To determine the relationship between self-selected walking speeds and gait symmetry in athletes after primary, unilateral ACLR.
Secondary analysis of a clinical trial.
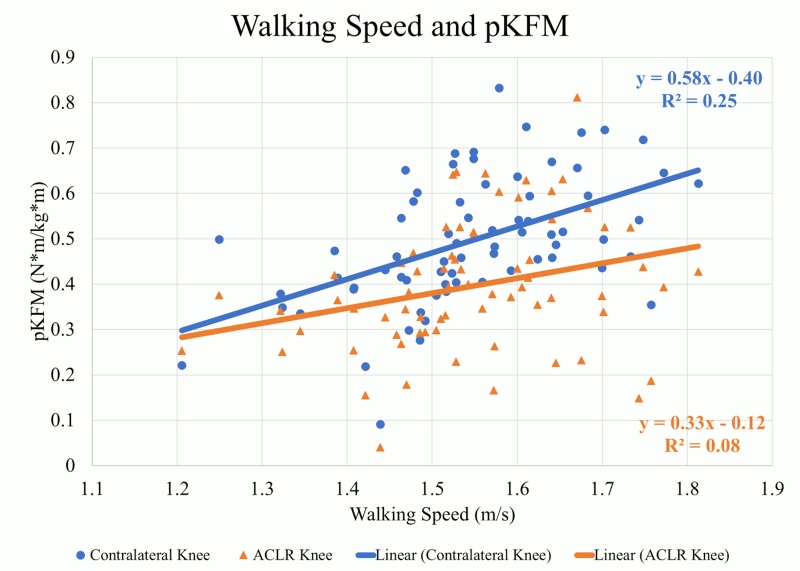
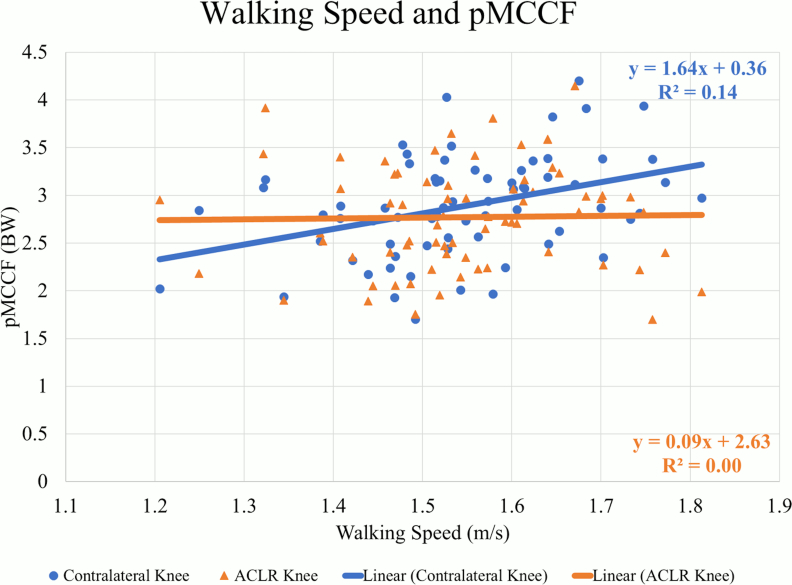
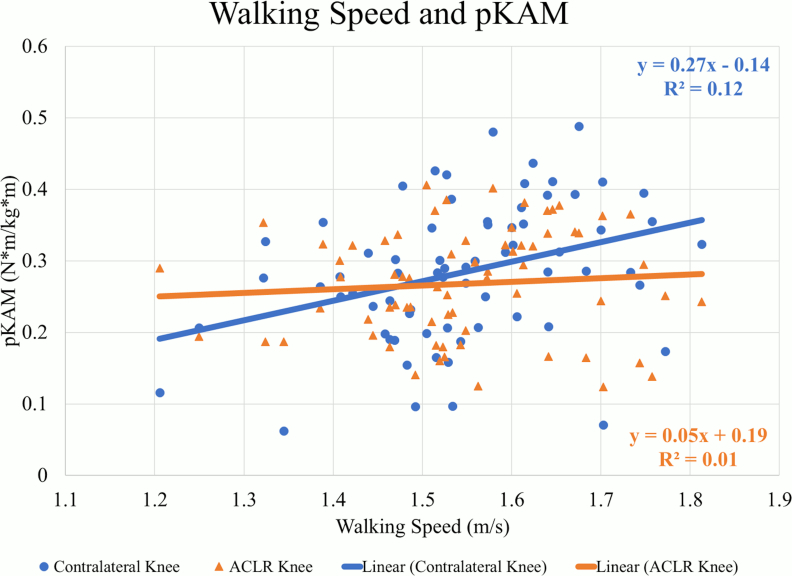
Athletes 24±8 weeks after primary ACLR walked at self-selected speeds as kinematics, kinetics, and electromyography data were collected. An EMG-driven musculoskeletal model was used to calculate peak medial compartment contact force (pMCCF). Variables of interest were peak knee flexion moment (pKFM) and angle (pKFA), knee flexion and extension (KEE) excursions, peak knee adduction moment (pKAM), and pMCCF. Univariate correlations were run for walking speed and each variable in the ACLR knee, contralateral knee, and interlimb difference (ILD).
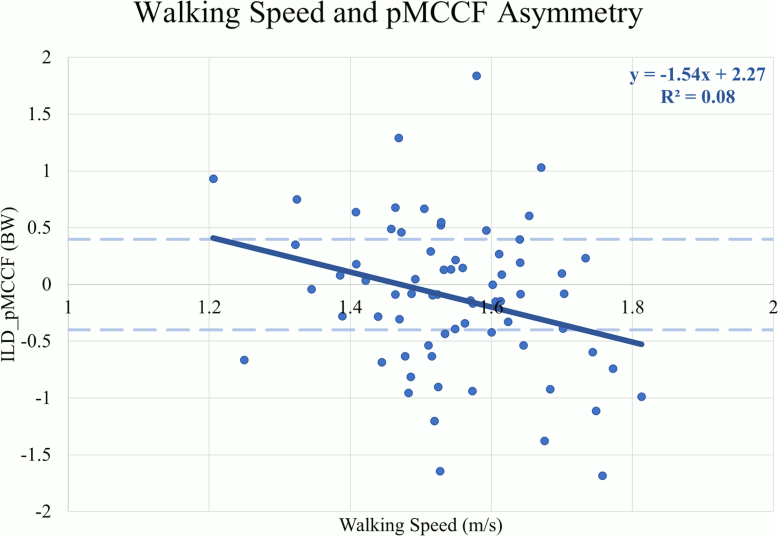
Weak to moderate positive correlations were observed for walking speed and all variables of interest in the contralateral knee (Pearson's r=.301-.505, p≤0.01). In the ACLR knee, weak positive correlations were observed for only pKFM (r=.280, p=0.02) and pKFA (r=.263, p=0.03). Weak negative correlations were found for ILDs in pKFM (r=-0.248, p=0.04), KEE (r=-.260, p=0.03), pKAM (r=-.323, p<0.01), and pMCCF (r=-.286, p=0.02).
Those who walk faster after ACLR have more asymmetries, which are associated with the development of early OA. This data suggests that interventions that solely increase walking speed may accentuate gait symmetry in athletes early after ACLR. Gait-specific, unilateral, neuromuscular interventions for the ACLR knee may be needed to target gait asymmetries after ACLR.
III.
前交叉韧带重建(ACLR)后步态不对称可能导致膝关节影像学骨关节炎。较慢的步行速度与提示软骨破坏的生物标志物有关。ACLR后步行速度与步态对称性之间的关系尚不清楚。
假设/目的:确定初次单侧ACLR后运动员自我选择的步行速度与步态对称性之间的关系。
一项临床试验的二次分析。
初次ACLR后24±8周的运动员以自我选择的速度行走,同时收集运动学、动力学和肌电图数据。使用肌电图驱动的肌肉骨骼模型计算内侧间室峰值接触力(pMCCF)。感兴趣的变量包括膝关节峰值屈曲力矩(pKFM)和角度(pKFA)、膝关节屈伸(KEE)偏移、膝关节峰值内收力矩(pKAM)和pMCCF。对ACLR侧膝关节、对侧膝关节以及双侧差值(ILD)的步行速度与每个变量进行单变量相关性分析。
在对侧膝关节中,观察到步行速度与所有感兴趣变量之间存在弱至中度正相关(Pearson相关系数r = 0.301 - 0.505,p≤0.01)。在ACLR侧膝关节中,仅pKFM(r = 0.280,p = 0.02)和pKFA(r = 0.263,p = 0.03)观察到弱正相关。在pKFM(r = -0.248,p = 0.04)、KEE(r = -0.260,p = 0.03)、pKAM(r = -0.323,p < 0.01)和pMCCF(r = -0.286,p = 0.02)的双侧差值中发现弱负相关。
ACLR后步行速度较快的人存在更多不对称性,这与早期骨关节炎的发展有关。该数据表明,单纯提高步行速度的干预措施可能会加重ACLR早期运动员的步态对称性。可能需要针对ACLR膝关节进行特定步态的单侧神经肌肉干预,以解决ACLR后的步态不对称问题。
III级。