Kristono Gisela A, Holley Ana S, Hally Kathryn E, Brunton-O'Sullivan Morgane M, Shi Bijia, Harding Scott A, Larsen Peter D
Department of Surgery and Anaesthesia, University of Otago Wellington, New Zealand.
Wellington Cardiovascular Research Group, New Zealand.
Cytokine X. 2020 Oct 8;2(4):100037. doi: 10.1016/j.cytox.2020.100037. eCollection 2020 Dec.
Many studies have shown that elevated biomarkers of inflammation following acute myocardial infarction (AMI) are associated with major adverse cardiovascular events (MACE). However, the optimal way of measuring the complex inflammatory response following AMI has not been determined. In this study we explore the use of principal component analysis (PCA) utilising multiple inflammatory cytokines to generate a combined cytokine score that may be predictive of MACE post-AMI.
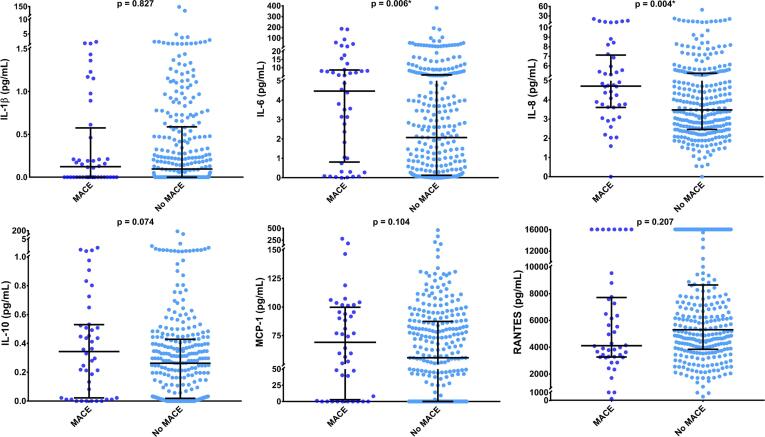
Thirteen inflammatory cytokines were measured in plasma of 317 AMI patients, drawn 48-72 h following symptom onset. Patients were followed-up for one year to determine the incidence of MACE. PCA was used to generate a combined score using six cytokines that were detectable in the majority of patients (IL-1β, -6, -8, and -10; MCP-1; and RANTES), and using a subset of cytokines that were associated with MACE on univariate analysis. Multivariate models using baseline characteristics, elevated individual cytokines and PCA-derived scores determined independent predictors of MACE.
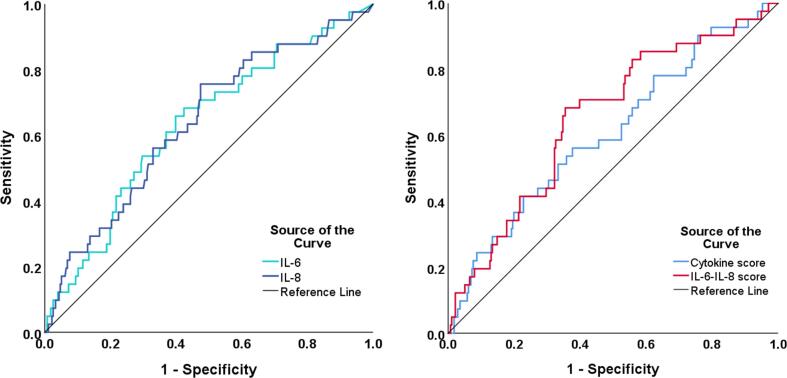
IL-6 and IL-8 were significantly associated with MACE on univariate analysis and were combined using PCA into an IL-6-IL-8 score. The combined cytokine score and IL-6-IL-8 PCA-derived score were both significantly associated with MACE on univariate analysis. In multivariate models IL-6-IL-8 scores (OR = 2.77, p = 0.007) and IL-6 levels (OR = 2.18, p = 0.035) were found to be independent predictors of MACE.
An IL-6-IL-8 score derived from PCA was found to independently predict MACE at one year and was a stronger predictor than any individual cytokine, which suggests this may be an appropriate strategy to quantify inflammation post-AMI. Further investigation is required to determine the optimal set of cytokines to measure in this context.
许多研究表明,急性心肌梗死(AMI)后炎症生物标志物升高与主要不良心血管事件(MACE)相关。然而,测量AMI后复杂炎症反应的最佳方法尚未确定。在本研究中,我们探索利用主成分分析(PCA),通过多种炎症细胞因子生成一个组合细胞因子评分,该评分可能预测AMI后的MACE。
在317例AMI患者症状发作后48 - 72小时采集的血浆中测量13种炎症细胞因子。对患者进行一年随访以确定MACE的发生率。PCA用于使用六种在大多数患者中可检测到的细胞因子(IL-1β、-6、-8和-10;MCP-1;和RANTES)生成组合评分,并使用单变量分析中与MACE相关的细胞因子子集。使用基线特征、升高的单个细胞因子和PCA衍生评分的多变量模型确定MACE的独立预测因素。
在单变量分析中,IL-6和IL-8与MACE显著相关,并通过PCA组合成IL-6 - IL-8评分。在单变量分析中,组合细胞因子评分和IL-6 - IL-8 PCA衍生评分均与MACE显著相关。在多变量模型中,发现IL-6 - IL-8评分(OR = 2.77,p = 0.007)和IL-6水平(OR = 2.18,p = 0.035)是MACE的独立预测因素。
发现通过PCA得出的IL-6 - IL-8评分可独立预测一年后的MACE,并且比任何单个细胞因子的预测能力更强,这表明这可能是量化AMI后炎症的合适策略。需要进一步研究以确定在此背景下测量的最佳细胞因子组合。