Department of Cardiology, Viborg Regional Hospital, Heibergs Alle 2K, 8800, Viborg, Denmark.
Department of Anaesthesiology and Intensive Care, Aarhus University Hospital, Aarhus, Denmark.
Scand J Trauma Resusc Emerg Med. 2021 Feb 19;29(1):37. doi: 10.1186/s13049-021-00849-7.
Transthoracic echocardiographic (TTE) indices of myocardial function among survivors of out-of-hospital cardiac arrest (OHCA) have been related to neurological outcome; however, results are inconsistent. We hypothesized that changes in average peak systolic mitral annular velocity (s') from 24 h (h) to 72 h following start of targeted temperature management (TTM) predict six-month neurological outcome in comatose OHCA survivors.
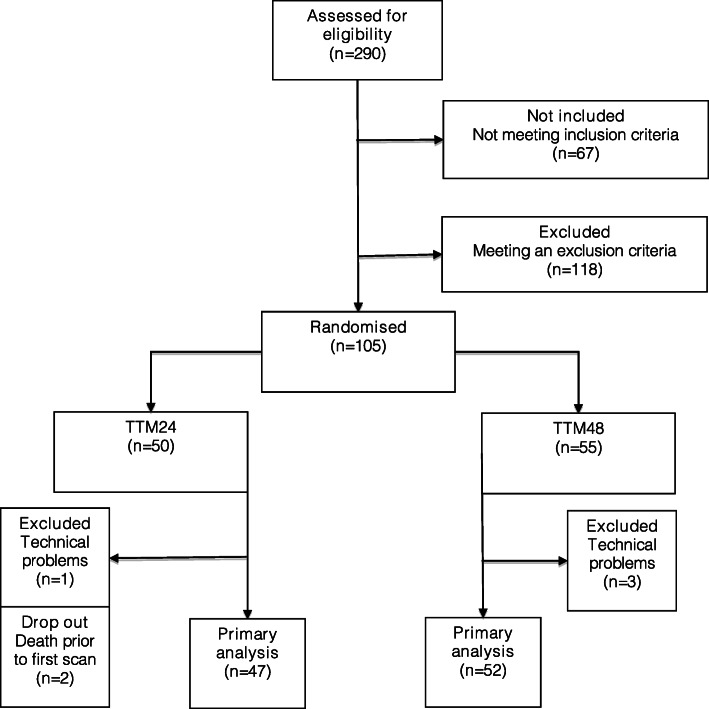
We investigated the association between peak systolic velocity of the mitral plane (s') and six-month neurological outcome in a population of 99 patients from a randomised controlled trial comparing TTM at 33 ± 1 °C for 24 h (h) (n = 47) vs. 48 h (n = 52) following OHCA (TTH48-trial). TTE was conducted at 24 h, 48 h, and 72 h after reaching target temperature. The primary outcome was 180 days neurological outcome assessed by Cerebral Performance Category score (CPC180) and the primary TTE outcome measure was s'. Secondary outcome measures were left ventricular ejection fraction (LVEF), global longitudinal strain (GLS), e', E/e' and tricuspid annular plane systolic excursion (TAPSE).
Across all three scan time points s' was not associated with neurological outcome (ORs: 24 h: 1.0 (95%CI: 0.7-1.4, p = 0.98), 48 h: 1.13 (95%CI: 0.9-1.4, p = 0.34), 72 h: 1.04 (95%CI: 0.8-1.4, p = 0.76)). LVEF, GLS, E/e', and TAPSE recorded on serial TTEs following OHCA were neither associated with nor did they predict CPC180. Estimated median e' at 48 h following TTM was 5.74 cm/s (95%CI: 5.27-6.22) in patients with good outcome (CPC180 1-2) vs. 4.95 cm/s (95%CI: 4.37-5.54) in patients with poor outcome (CPC180 3-5) (p = 0.04).
s' assessed on serial TTEs in comatose survivors of OHCA treated with TTM was not associated with CPC180. Our findings suggest that serial TTEs in the early post-resuscitation phase during TTM do not aid the prognostication of neurological outcome following OHCA.
NCT02066753 . Registered 14 February 2014 - Retrospectively registered.
在院外心脏骤停(OHCA)幸存者中,经胸超声心动图(TTE)心肌功能指标与神经结局相关;然而,结果并不一致。我们假设,从开始目标温度管理(TTM)后 24 小时(h)到 72 小时(h)平均收缩期二尖瓣环速度峰值(s')的变化可以预测昏迷 OHCA 幸存者的 6 个月神经结局。
我们研究了 99 名随机对照试验患者的峰值收缩速度(s')与 6 个月神经结局之间的关联,该试验比较了 TTM 在 33±1°C 持续 24 h(n=47)与 48 h(n=52)后的比较(TTH48 试验)。在达到目标温度后 24、48 和 72 h 进行 TTE。主要结局是由脑功能分类评分(CPC180)评估的 180 天神经结局,主要 TTE 结局测量指标是 s'。次要结局测量指标包括左心室射血分数(LVEF)、整体纵向应变(GLS)、e'、E/e'和三尖瓣环平面收缩期位移(TAPSE)。
在所有三个扫描时间点,s'均与神经结局无关(OR:24 h:1.0(95%CI:0.7-1.4,p=0.98),48 h:1.13(95%CI:0.9-1.4,p=0.34),72 h:1.04(95%CI:0.8-1.4,p=0.76))。OHCA 后连续 TTE 记录的 LVEF、GLS、E/e'和 TAPSE 均与 CPC180 无关,也无法预测 CPC180。TTM 后 48 h 时,估计的中位 e'在结局良好(CPC180 1-2)的患者中为 5.74 cm/s(95%CI:5.27-6.22),在结局较差(CPC180 3-5)的患者中为 4.95 cm/s(95%CI:4.37-5.54)(p=0.04)。
在接受 TTM 治疗的 OHCA 昏迷幸存者中,连续 TTE 评估的 s'与 CPC180 无关。我们的研究结果表明,TTM 后复苏早期的连续 TTE 无助于预测 OHCA 后的神经结局。
NCT02066753。于 2014 年 2 月 14 日注册-回顾性注册。