Takemi Program in International Health, Harvard T.H. Chan School of Public Health, Harvard University.
Department of Economic History, School of Economics and Management, Lund University.
J Epidemiol. 2022 Jul 5;32(7):337-344. doi: 10.2188/jea.JE20200537. Epub 2021 Jul 10.
Prevalence of stunting is frequently used as a marker of population-level child undernutrition. Parental height varies widely in low- and middle-income countries (LMIC) and is also a major determinant of stunting. While stunting is a useful measure of child health, with multiple causal components, removing the component attributable to parental height may in some cases be helpful to identify shortcoming in current environments.
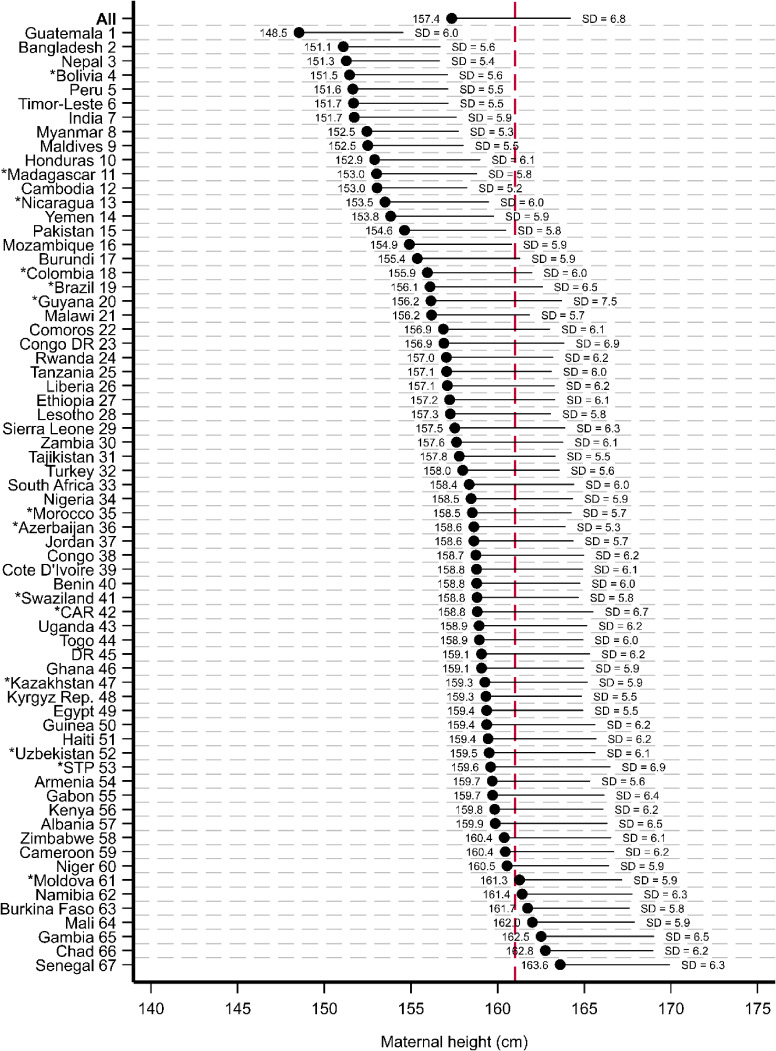
We estimated maternal height-standardized prevalence of stunting (SPS) in 67 LMICs and parental height-SPS in 20 LMICs and compared with crude prevalence of stunting (CPS) using data on 575,767 children under-five from 67 Demographic and Health Surveys (DHS). We supplemented the DHS with population-level measures of other child health outcomes from the World Health Organization's (WHO) Global Health Observatory and the United Nations' Inter-Agency Group for Child Mortality Estimation. Prevalence of stunting was defined as percentage of children with height-for-age falling below -2 z-scores from the median of the 2006 WHO growth standard.
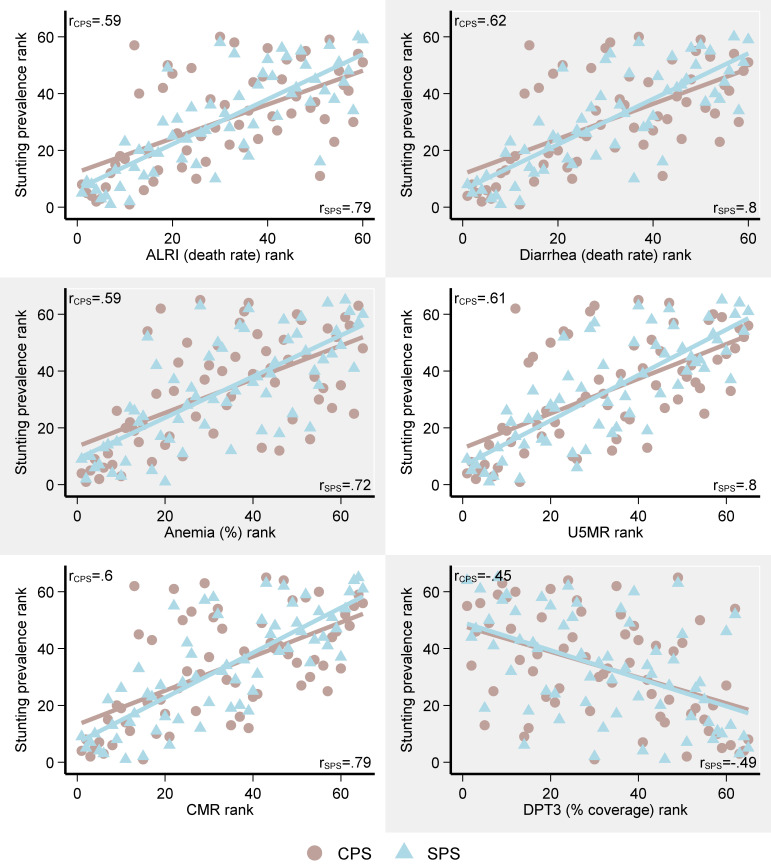
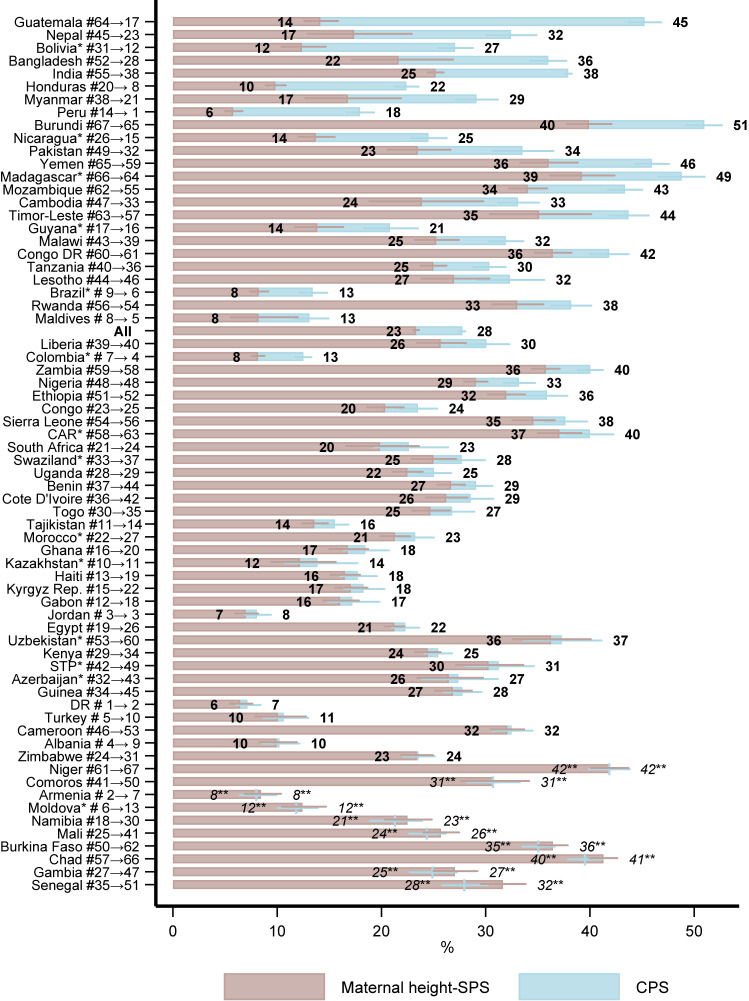
The average CPS across countries was 27.8% (95% confidence interval [CI], 27.5-28.1%) and the average SPS was 23.3% (95% CI, 23.0-23.6%). The rank of countries according to SPS differed substantially from the rank according to CPS. Guatemala, Bangladesh, and Nepal had the biggest improvement in ranking according to SPS compared to CPS, while Gambia, Mali, and Senegal had the biggest decline in ranking. Guatemala had the largest difference between CPS and SPS with a CPS of 45.2 (95% CI, 43.7-46.9%) and SPS of 14.1 (95% CI, 12.6-15.8%). Senegal had the largest increase in the prevalence after standardizing maternal height, with a CPS of 28.0% (95% CI, 25.8-30.2%) and SPS of 31.6% (95% CI, 29.5-33.8%). SPS correlated better than CPS with other population-level measures of child health.
Our study suggests that CPS is sensitive to adjustment for maternal height. Maternal height, while a strong predictor of child stunting, is not amenable to policy interventions. We showed the plausibility of SPS in capturing current exposures to undernutrition and infections in children.
发育迟缓的流行率常被用作人群层面儿童营养不良的指标。在低收入和中等收入国家(LMIC),父母的身高差异很大,也是发育迟缓的主要决定因素。虽然发育迟缓是衡量儿童健康的一个有用指标,有多个因果因素,但消除与父母身高相关的因素,在某些情况下可能有助于发现当前环境中的不足之处。
我们估计了 67 个 LMIC 国家的母亲身高标准化发育迟缓患病率(SPS)和 20 个 LMIC 国家的父母身高-SPS,并使用来自 67 项人口与健康调查(DHS)的 575767 名五岁以下儿童的数据,将其与发育迟缓的粗患病率(CPS)进行比较。我们使用世界卫生组织(WHO)全球卫生观察站和联合国儿童死亡率估计机构间小组的其他儿童健康结果的人口水平指标补充 DHS。发育迟缓的患病率定义为身高低于年龄中位数 -2 z 分数的儿童百分比,来自 2006 年 WHO 生长标准。
各国平均 CPS 为 27.8%(95%置信区间[CI],27.5-28.1%),平均 SPS 为 23.3%(95% CI,23.0-23.6%)。根据 SPS 的国家排名与根据 CPS 的国家排名有很大差异。危地马拉、孟加拉国和尼泊尔根据 SPS 的排名上升幅度最大,而冈比亚、马里和塞内加尔的排名下降幅度最大。危地马拉的 CPS 和 SPS 之间的差异最大,CPS 为 45.2%(95% CI,43.7-46.9%),SPS 为 14.1%(95% CI,12.6-15.8%)。塞内加尔在调整母亲身高后,发育迟缓的患病率增幅最大,CPS 为 28.0%(95% CI,25.8-30.2%),SPS 为 31.6%(95% CI,29.5-33.8%)。SPS 与其他人群层面的儿童健康指标比 CPS 相关性更好。
我们的研究表明,CPS 对母亲身高的调整很敏感。母亲身高虽然是儿童发育迟缓的一个强有力的预测因素,但无法进行政策干预。我们展示了 SPS 在捕捉儿童当前营养不足和感染暴露方面的可行性。