Lancet Child Adolesc Health. 2019 Dec;3(12):855-870. doi: 10.1016/S2352-4642(19)30273-1. Epub 2019 Sep 18.
Malnutrition is a major contributor to disease burden in India. To inform subnational action, we aimed to assess the disease burden due to malnutrition and the trends in its indicators in every state of India in relation to Indian and global nutrition targets.
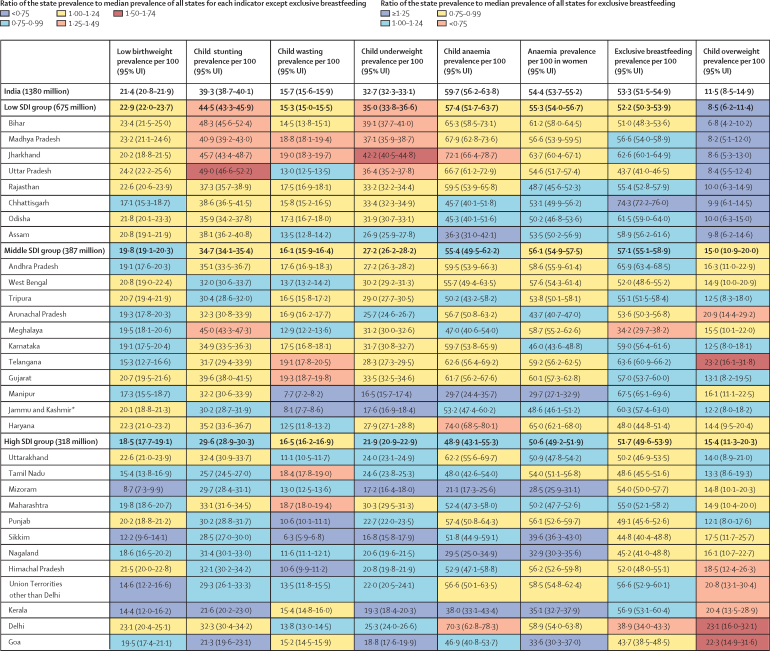
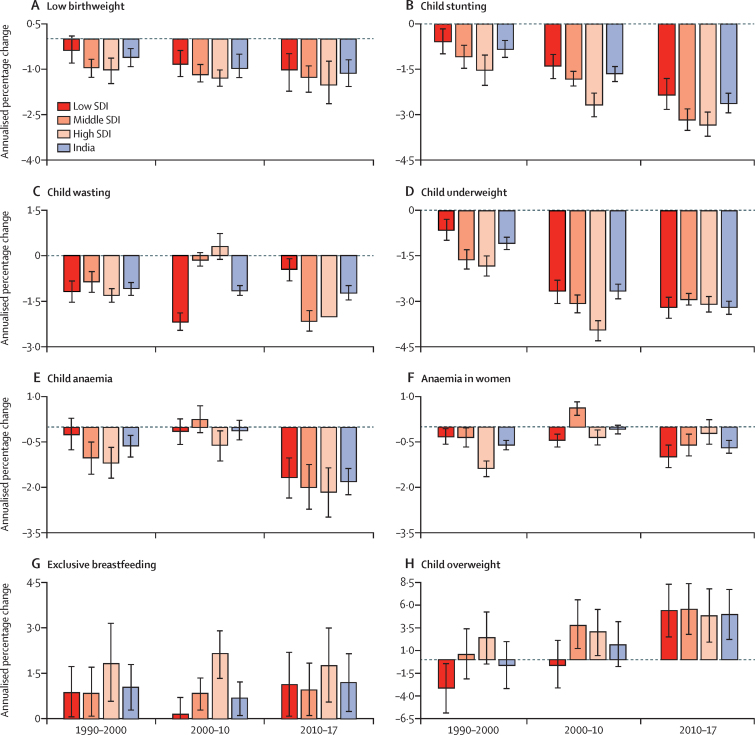
We analysed the disease burden attributable to child and maternal malnutrition, and the trends in the malnutrition indicators from 1990 to 2017 in every state of India using all accessible data from multiple sources, as part of Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2017. The states were categorised into three groups using their Socio-demographic Index (SDI) calculated by GBD on the basis of per capita income, mean education, and fertility rate in women younger than 25 years. We projected the prevalence of malnutrition indicators for the states of India up to 2030 on the basis of the 1990-2017 trends for comparison with India National Nutrition Mission (NNM) 2022 and WHO and UNICEF 2030 targets.
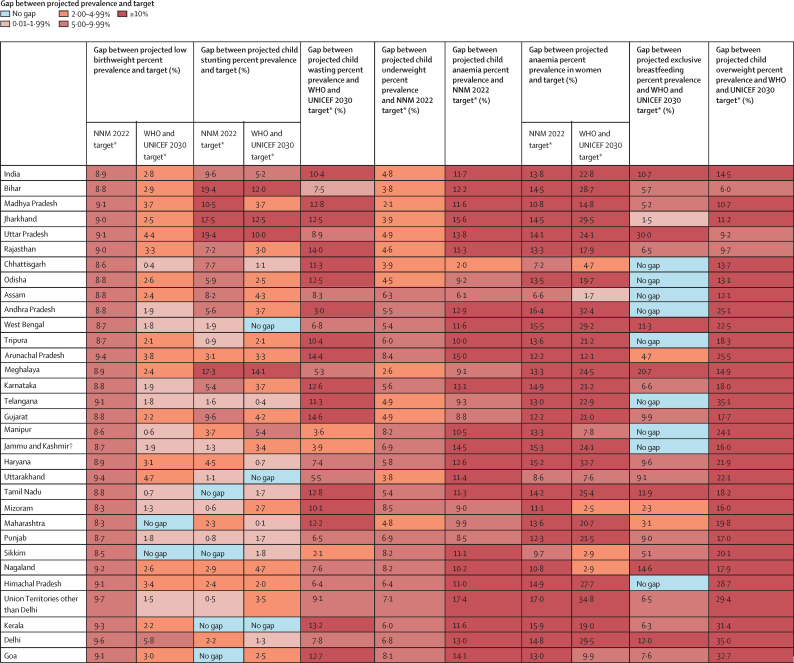
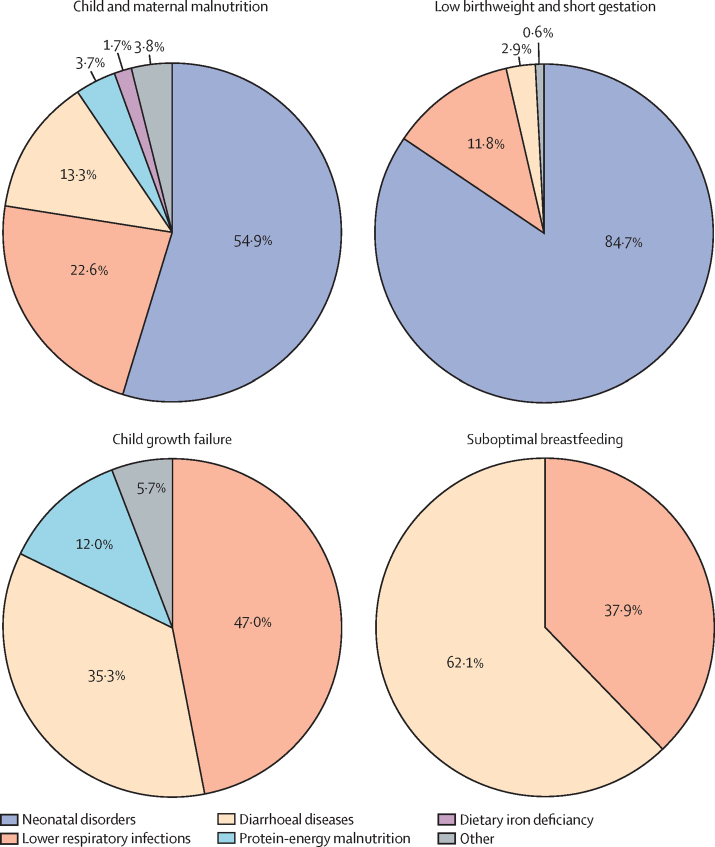
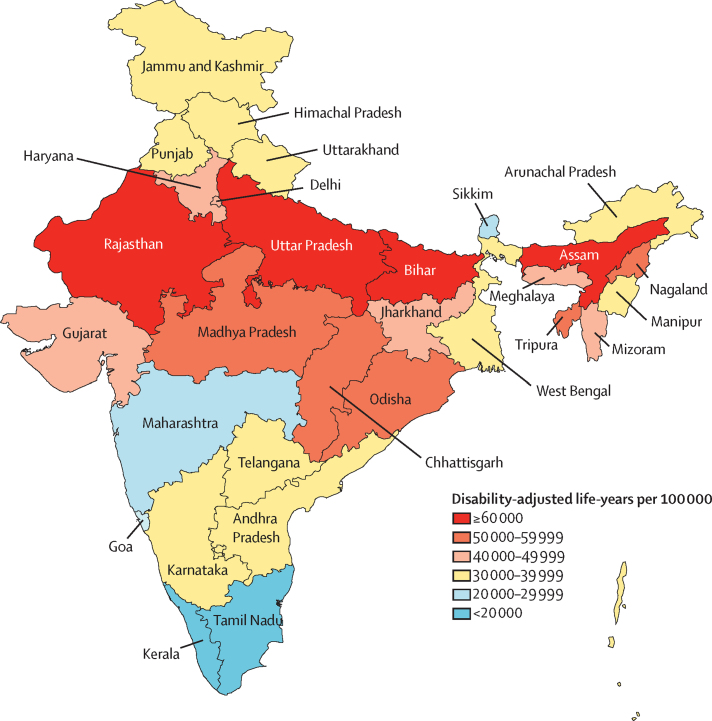
Malnutrition was the predominant risk factor for death in children younger than 5 years of age in every state of India in 2017, accounting for 68·2% (95% UI 65·8-70·7) of the total under-5 deaths, and the leading risk factor for health loss for all ages, responsible for 17·3% (16·3-18·2) of the total disability-adjusted life years (DALYs). The malnutrition DALY rate was much higher in the low SDI than in the middle SDI and high SDI state groups. This rate varied 6·8 times between the states in 2017, and was highest in the states of Uttar Pradesh, Bihar, Assam, and Rajasthan. The prevalence of low birthweight in India in 2017 was 21·4% (20·8-21·9), child stunting 39·3% (38·7-40·1), child wasting 15·7% (15·6-15·9), child underweight 32·7% (32·3-33·1), anaemia in children 59·7% (56·2-63·8), anaemia in women 15-49 years of age 54·4% (53·7-55·2), exclusive breastfeeding 53·3% (51·5-54·9), and child overweight 11·5% (8·5-14·9). If the trends estimated up to 2017 for the indicators in the NNM 2022 continue in India, there would be 8·9% excess prevalence for low birthweight, 9·6% for stunting, 4·8% for underweight, 11·7% for anaemia in children, and 13·8% for anaemia in women relative to the 2022 targets. For the additional indicators in the WHO and UNICEF 2030 targets, the trends up to 2017 would lead to 10·4% excess prevalence for wasting, 14·5% excess prevalence for overweight, and 10·7% less exclusive breastfeeding in 2030. The prevalence of malnutrition indicators, their rates of improvement, and the gaps between projected prevalence and targets vary substantially between the states.
Malnutrition continues to be the leading risk factor for disease burden in India. It is encouraging that India has set ambitious targets to reduce malnutrition through NNM. The trends up to 2017 indicate that substantially higher rates of improvement will be needed for all malnutrition indicators in most states to achieve the Indian 2022 and the global 2030 targets. The state-specific findings in this report indicate the effort needed in each state, which will be useful in tracking and motivating further progress. Similar subnational analyses might be useful for other low-income and middle-income countries.
Bill & Melinda Gates Foundation; Indian Council of Medical Research, Department of Health Research, Ministry of Health and Family Welfare, Government of India.
营养不良是印度疾病负担的主要原因之一。为了为国家行动提供信息,我们旨在评估印度每个邦的营养不良相关疾病负担以及营养不良指标的趋势,同时考虑到印度和全球的营养目标。
我们分析了儿童和孕产妇营养不良的疾病负担,以及 1990 年至 2017 年期间印度每个邦的营养不良指标的变化趋势,这些数据来自全球疾病、伤害和风险因素研究(GBD)2017 中的多个来源。根据 GBD 基于人均收入、平均教育水平和 25 岁以下女性生育率计算的社会发展指数(SDI),将各州分为三组。我们根据 1990-2017 年的趋势预测了印度各州的营养不良指标的患病率,以便与印度国家营养使命(NNM)2022 年和世界卫生组织(WHO)和联合国儿童基金会(UNICEF)2030 年的目标进行比较。
在 2017 年,营养不良是印度每个邦 5 岁以下儿童死亡的主要原因,占总 5 岁以下儿童死亡人数的 68.2%(95%UI 65.8-70.7),也是所有年龄段健康损失的主要风险因素,占总残疾调整生命年(DALY)的 17.3%(16.3-18.2)。在低 SDI 州组中,营养不良的 DALY 率要高得多。2017 年,各州之间的这一比率相差 6.8 倍,最高的是北方邦、比哈尔邦、阿萨姆邦和拉贾斯坦邦。2017 年印度的低出生体重率为 21.4%(20.8-21.9),儿童发育迟缓率为 39.3%(38.7-40.1),儿童消瘦率为 15.7%(15.6-15.9),儿童体重不足率为 32.7%(32.3-33.1),儿童贫血率为 59.7%(56.2-63.8),15-49 岁妇女贫血率为 54.4%(53.7-55.2),纯母乳喂养率为 53.3%(51.5-54.9),儿童超重率为 11.5%(8.5-14.9)。如果按照 NNM 2022 年的指标趋势估计到 2017 年,那么低出生体重将增加 8.9%,发育迟缓将增加 9.6%,体重不足将增加 4.8%,儿童贫血将增加 11.7%,妇女贫血将增加 13.8%,与 2022 年的目标相比。对于 WHO 和 UNICEF 2030 年目标中的其他指标,到 2017 年的趋势将导致消瘦率增加 10.4%,超重率增加 14.5%,2030 年纯母乳喂养率降低 10.7%。
各州的营养不良指标的流行率、改善率以及与目标的差距差异很大。
营养不良仍然是印度疾病负担的主要原因。令人鼓舞的是,印度已经制定了雄心勃勃的目标,通过 NNM 来减少营养不良。截至 2017 年的趋势表明,大多数州需要更高的改善率,才能实现印度 2022 年和全球 2030 年的目标。本报告中的州级发现表明了每个州需要做出的努力,这将有助于跟踪和激励进一步的进展。类似的国家内分析可能对其他低收入和中等收入国家有用。
比尔及梅琳达·盖茨基金会;印度医学研究理事会,印度卫生部,印度家庭福利部,印度政府。