Ghosh Santu, Shivakumar Nirupama, Bandyopadhyay Sulagna, Sachdev Harshpal S, Kurpad Anura V, Thomas Tinku
Department of Biostatistics, St. John's Medical College, St. John's Academy of Health Sciences, Bangalore, 560034, India.
Division of Nutrition, St. John's Research Institute, St. John's Academy of Health Sciences, Bangalore, India.
BMC Public Health. 2020 Nov 1;20(1):1634. doi: 10.1186/s12889-020-09753-8.
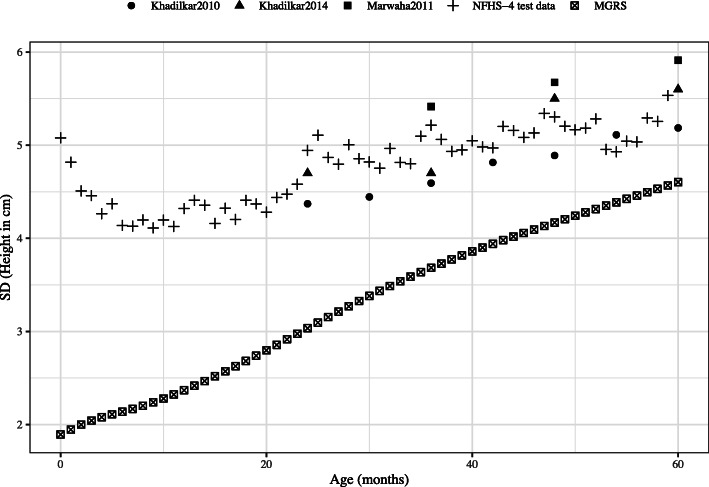
Stunting is determined by using the World Health Organization (WHO) child growth standard which was developed using precise measurements. However, it is unlikely that large scale surveys maintain the same level of rigour and precision when measuring the height of children. The population measure of stunting in children is sensitive to over-dispersion, and the high prevalence of stunting observed in surveys in low and middle-income countries (LMIC) could partly be due to lower measurement precison.
To quantify the incongruence in the dispersion of height-for-age in national surveys of < 5 y children, in relation to the standard WHO Multicenter Growth Reference Study (MGRS), and propose a measure of uncertainty in population measures of stunting.
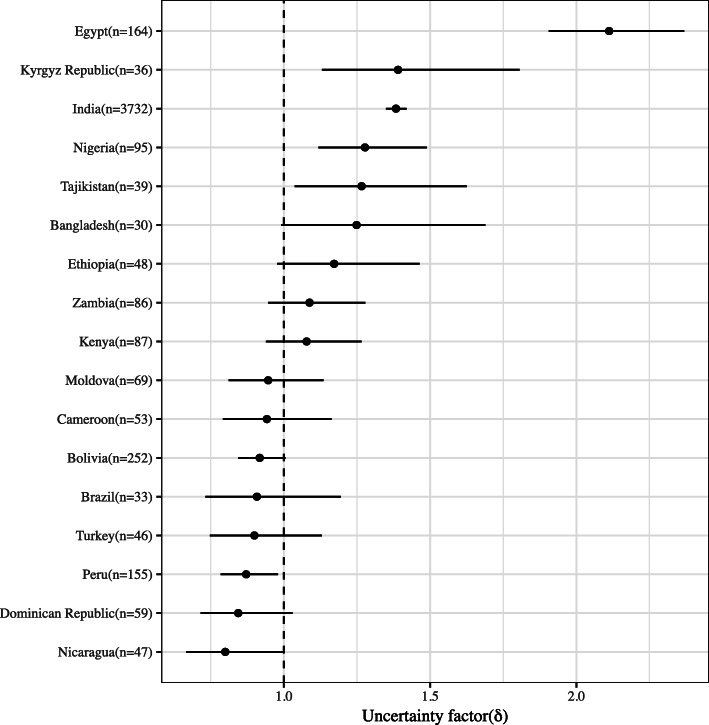
An uncertainty factor was proposed and measured from the observed incongruence in dispersion of the height-for-age of < 5 y children in the MGRS against carefully matched populations from the Demographic Health Survey of 17 countries ('test datasets', based on the availability of data). This also allowed for the determination of uncertainty-corrected prevalence of stunting (height-for-age Z score < - 2) in < 5 y children.
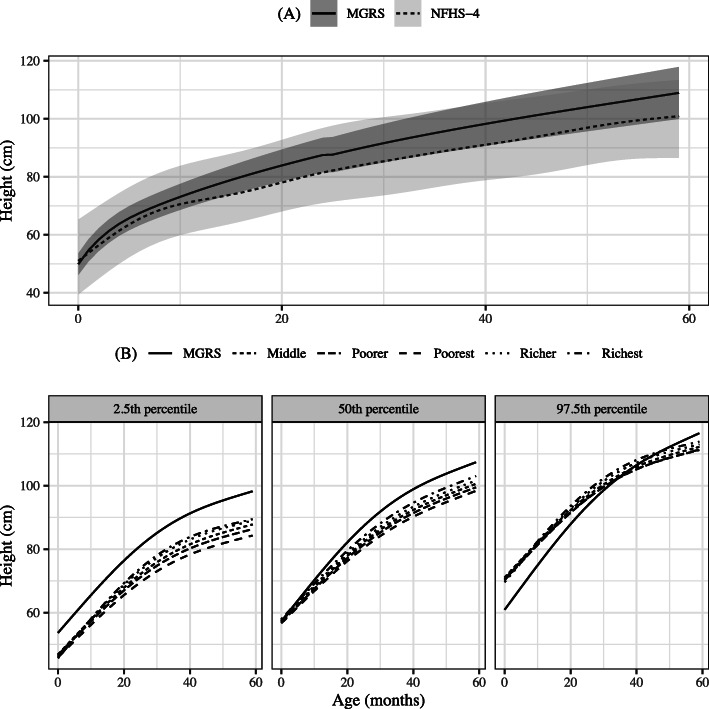
The uncertainty factor was estimated for 17 LMICs. This ranged from 0.9 to 2.1 for Peru and Egypt respectively (reference value 1). As an explicit country example, the dispersion of height-for-age in the Indian National Family Health Survey-4 test dataset was 39% higher than the MGRS study, with an uncertainty factor of 1.39. From this, the uncertainty-adjusted Indian national stunting prevalence estimate reduced to 18.7% from the unadjusted estimate of 36.2%.
This study proposes a robust statistical method to estimate uncertainty in stunting prevalence estimates due to incongruent dispersions of height measured in national surveys for children < 5 years in relation to the WHO height-for-age standard. The uncertainty is partly due to population heterogeneity, but also due to measurement precision, and calls for better quality in these measurements.
发育迟缓是通过使用世界卫生组织(WHO)的儿童生长标准来确定的,该标准是通过精确测量制定的。然而,在大规模调查中测量儿童身高时,不太可能保持相同程度的严谨性和精确性。儿童发育迟缓的总体衡量指标对过度离散很敏感,在低收入和中等收入国家(LMIC)的调查中观察到的高发育迟缓患病率可能部分归因于较低的测量精度。
量化5岁以下儿童全国性调查中年龄别身高离散度与WHO多中心生长参考研究(MGRS)标准之间的不一致性,并提出一种衡量发育迟缓总体指标不确定性的方法。
提出并测量了一个不确定性因素,该因素基于MGRS中5岁以下儿童年龄别身高的观察离散度与17个国家人口与健康调查中精心匹配的人群(“测试数据集”,取决于数据可用性)之间的不一致性。这也有助于确定5岁以下儿童发育迟缓(年龄别身高Z评分<-2)的不确定性校正患病率。
估计了17个低收入和中等收入国家的不确定性因素。秘鲁和埃及的该因素分别为0.9至2.1(参考值为1)。作为一个明确的国家示例,印度第四次全国家庭健康调查测试数据集中年龄别身高的离散度比MGRS研究高39%,不确定性因素为1.39。据此,印度全国发育迟缓患病率的不确定性调整估计值从未调整的36.2%降至18.7%。
本研究提出了一种稳健的统计方法,用于估计在全国性调查中测量的5岁以下儿童身高离散度与WHO年龄别身高标准不一致导致的发育迟缓患病率估计值的不确定性。这种不确定性部分归因于人群异质性,但也归因于测量精度,因此需要提高这些测量的质量。