Centre for Reproductive Medicine, Amsterdam UMC, Location Academic Medical Centre, 1105 AZ Amsterdam, the Netherlands.
Department of Obstetrics and Gynaecology, Monash University, Clayton, VIC 3168, Australia.
Hum Reprod. 2021 Apr 20;36(5):1288-1295. doi: 10.1093/humrep/deab013.
Which agent for ovarian stimulation (OS) is the most cost-effective option in terms of net benefit for couples with unexplained subfertility undergoing IUI?
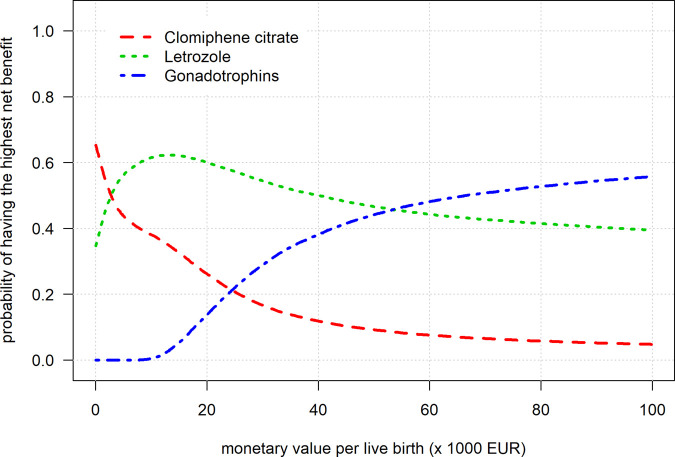
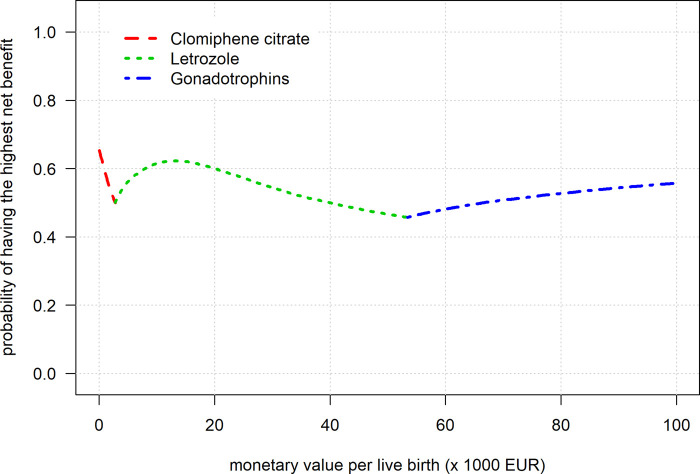
In settings where a live birth is valued at €3000 or less, between €3000 and €55 000 and above €55 000, clomiphene citrate (CC), Letrozole and gonadotrophins were the most cost-effective option in terms of net benefit, respectively.
IUI-OS is a common first-line treatment for couples with unexplained subfertility and its increased uptake over the past decades and related personal or reimbursed costs are pressing concerns to patients and health service providers. However, there is no consensus on a protocol for conducting IUI-OS, with differences between countries, clinics and settings in the number of cycles, success rates, the agent for OS and the maximum number of dominant follicles in order to minimise the risk of a multiple pregnancy. In view of this uncertainty and the association with costs, guidance is needed on the cost-effectiveness of OS agents for IUI-OS.
STUDY DESIGN, SIZE, DURATION: We developed a decision-analytic model based on a decision tree that follows couples with unexplained subfertility from the start of IUI-OS to a protocoled maximum of six cycles, assuming couples receive four cycles on average within one year. We chose the societal perspective, which coincides with other perspectives such as that from health care providers, as the treatments are identical except for the stimulation agent. We based our model on parameters from a network meta-analysis of randomised controlled trials for IUI-OS. We compared the following three agents: CC (oral medication), Letrozole (oral medication) and gonadotrophins (subcutaneous injection).
PARTICIPANTS/MATERIALS, SETTING, METHODS: The main health outcomes were cumulative live birth and multiple pregnancy. As the procedures are identical except for the agent used, we only considered direct medical costs of the agent during four cycles. The main cost-effectiveness measures were the differences in costs divided by the differences in cumulative live birth (incremental cost-effectiveness ratio, ICER) and the probability of the highest net monetary benefit in which costs for an agent were deducted from the live births gained. The live birth rate for IUI using CC was taken from trials adhering to strict cancellation criteria included in a network meta-analysis and extrapolated to four cycles. We took the relative risks for the live birth rate after Letrozole and gonadotrophins versus CC from that same network meta-analysis to estimate the remaining absolute live birth rates. The uncertainty around live birth rates, relative effectiveness and costs was assessed by probabilistic sensitivity analysis in which we drew values from distributions and repeated this procedure 20 000 times. In addition, we changed model assumptions to assess their influence on our results.
The agent with the lowest cumulative live birth rate over 4 IUI-OS cycles conducted within one year was CC (29.4%), followed by Letrozole (32.0%) and gonadotrophins (34.5%). The average costs per four cycles were €362, €434 and €1809, respectively. The ICER of Letrozole versus CC was €2809 per additional live birth, whereas the ICER of gonadotrophins versus Letrozole was €53 831 per additional live birth. When we assume a live birth is valued at €3000 or less, CC had the highest probability of maximally 65% to achieve the highest net benefit. Between €3000 and €55 000, Letrozole had the highest probability of maximally 62% to achieve the highest net benefit. Assuming a monetary value of €55 000 or more, gonadotrophins had the highest probability of maximally 56% to achieve the highest net benefit.
LIMITATIONS, REASONS FOR CAUTION: Our model focused on population level and was thus based on average costs for the average number of four cycles conducted. We also based the model on a number of key assumptions. We changed model assumptions to assess the influence of these assumptions on our results.
The high uncertainty surrounding our results indicate that more research is necessary on the relative effectiveness of using CC, Letrozole or gonadotrophins for IUI-OS in terms of the cumulative live birth rate. We suggest that in the meantime, CC or Letrozole are the preferred choice of agent.
STUDY FUNDING/COMPETING INTEREST(S): This work was supported by ZonMw Doelmatigheidsonderzoek, grant 80-85200-98-91072. The funder had no role in the design, conduct or reporting of this work. BWM is supported by a NHMRC Practitioner Fellowship (GNT1082548). B.W.M. reports consultancy for ObsEva, Merck KGaA and Guerbet and travel and research support from ObsEva, Merck and Guerbet. All other authors have no conflicts of interest to declare.
N/A.
对于不明原因的不孕夫妇进行 IUI,哪种促排卵(OS)药物在净效益方面最具成本效益?
在活产价值低于或等于 3000 欧元、3000 欧元至 55000 欧元和高于 55000 欧元的情况下,分别是氯米酚、来曲唑和促性腺激素最具成本效益。
IUI-OS 是不明原因不孕夫妇的一种常见一线治疗方法,过去几十年来,它的应用越来越广泛,以及与之相关的个人或报销费用,是患者和医疗服务提供者关注的焦点。然而,在进行 IUI-OS 的方案方面尚无共识,不同国家、诊所和环境之间在周期数、成功率、OS 药物和最大数量的优势卵泡方面存在差异,以尽量降低多胎妊娠的风险。鉴于这种不确定性以及与成本的关联,需要对 IUI-OS 的 OS 药物的成本效益进行指导。
研究设计、规模、持续时间:我们开发了一个基于决策树的决策分析模型,该模型遵循不明原因不孕夫妇的情况,从 IUI-OS 开始到协议规定的最多六个周期,假设夫妇平均在一年内接受四个周期的治疗。我们选择了社会视角,这与医疗保健提供者的视角等其他视角一致,因为除了刺激药物外,治疗方法是相同的。我们的模型基于对 IUI-OS 的随机对照试验网络荟萃分析的参数。我们比较了以下三种药物:氯米酚(口服药物)、来曲唑(口服药物)和促性腺激素(皮下注射)。
参与者/材料、设置、方法:主要的健康结果是累积活产和多胎妊娠。由于除了药物之外,程序是相同的,我们只考虑了四个周期内药物的直接医疗成本。主要的成本效益衡量标准是成本差异除以累积活产的差异(增量成本效益比,ICER)以及扣除活产收益的药物成本后的最高净货币收益的概率。使用氯米酚的 IUI 活产率是从包括在网络荟萃分析中的严格取消标准的试验中获得的,并外推到四个周期。我们从同一网络荟萃分析中获得了来曲唑和促性腺激素与氯米酚的活产率的相对风险,以估计剩余的绝对活产率。通过从分布中抽取值并重复该过程 20000 次来评估活产率、相对有效性和成本的不确定性。此外,我们还改变了模型假设,以评估它们对结果的影响。
在一年内进行的四个 IUI-OS 周期内,累积活产率最低的药物是氯米酚(29.4%),其次是来曲唑(32.0%)和促性腺激素(34.5%)。四个周期的平均成本分别为 362 欧元、434 欧元和 1809 欧元。来曲唑与氯米酚相比的 ICER 为 2809 欧元/额外活产,而促性腺激素与来曲唑相比的 ICER 为 53831 欧元/额外活产。当我们假设活产价值低于或等于 3000 欧元时,氯米酚实现最高净效益的概率最高可达 65%。在 3000 欧元至 55000 欧元之间,来曲唑实现最高净效益的概率最高可达 62%。假设货币价值为 55000 欧元或更高,促性腺激素实现最高净效益的概率最高可达 56%。
局限性、谨慎的原因:我们的模型侧重于人群水平,因此是基于平均成本和平均 4 个周期的数量。我们还基于一些关键假设构建了模型。我们改变了模型假设,以评估这些假设对结果的影响。
我们的研究结果存在很高的不确定性,这表明在 IUI-OS 中使用氯米酚、来曲唑或促性腺激素的累积活产率方面,需要进行更多的相对有效性研究。我们建议在此期间,氯米酚或来曲唑是首选药物。
研究资助/利益冲突:这项工作得到了 ZonMw 目标研究的支持,拨款 80-85200-98-91072。资助者在研究的设计、进行或报告中没有作用。BWM 得到了 NHMRC 从业者奖学金(GNT1082548)的支持。B.W.M. 报告了与 ObsEva、默克公司和 Guerbet 的咨询服务以及与 ObsEva、默克公司和 Guerbet 的旅行和研究支持。所有其他作者均无利益冲突声明。
无。