Amsterdam UMC location University of Amsterdam, Centre for Reproductive Medicine, Department of Obstetrics and Gynaecology, Amsterdam Reproduction and Development Research Institute, Meibergdreef 9, 1105 AZ, Amsterdam, The Netherlands.
Department of Obstetrics and Gynecology, Augusta University, Augusta, GA 30912, USA.
Hum Reprod Update. 2022 Aug 25;28(5):733-746. doi: 10.1093/humupd/dmac021.
Intrauterine insemination with ovarian stimulation (IUI-OS) is a first-line treatment for unexplained infertility. Gonadotrophins, letrozole and clomiphene citrate (CC) are commonly used agents during IUI-OS and have been compared in multiple aggregate data meta-analyses, with substantial heterogeneity and no analysis on time-to-event outcomes. Individual participant data meta-analysis (IPD-MA) is considered the gold standard for evidence synthesis as it can offset inadequate reporting of individual studies by obtaining the IPD, and allows analyses on treatment-covariate interactions to identify couples who benefit most from a particular treatment.
We performed this IPD-MA to compare the effectiveness and safety of ovarian stimulation with gonadotrophins, letrozole and CC and to explore treatment-covariate interactions for important baseline characteristics in couples undergoing IUI.
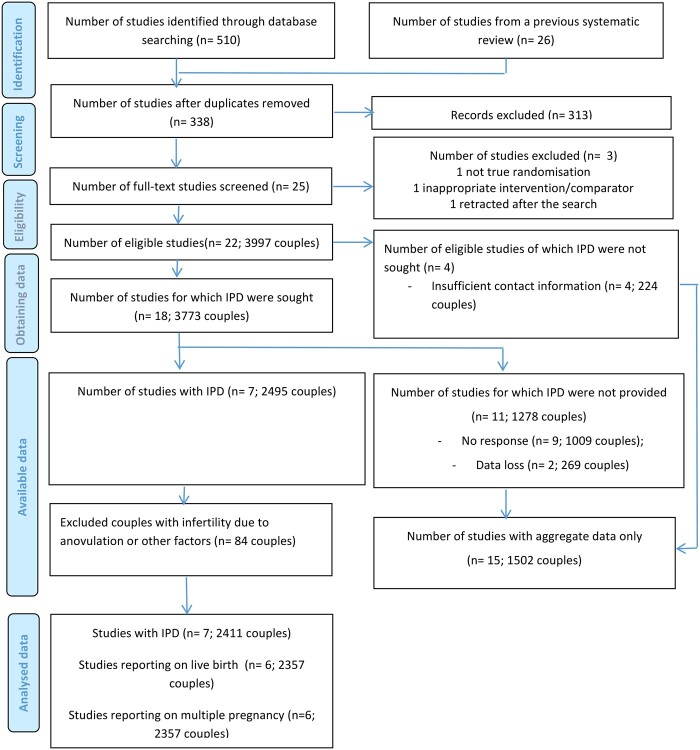
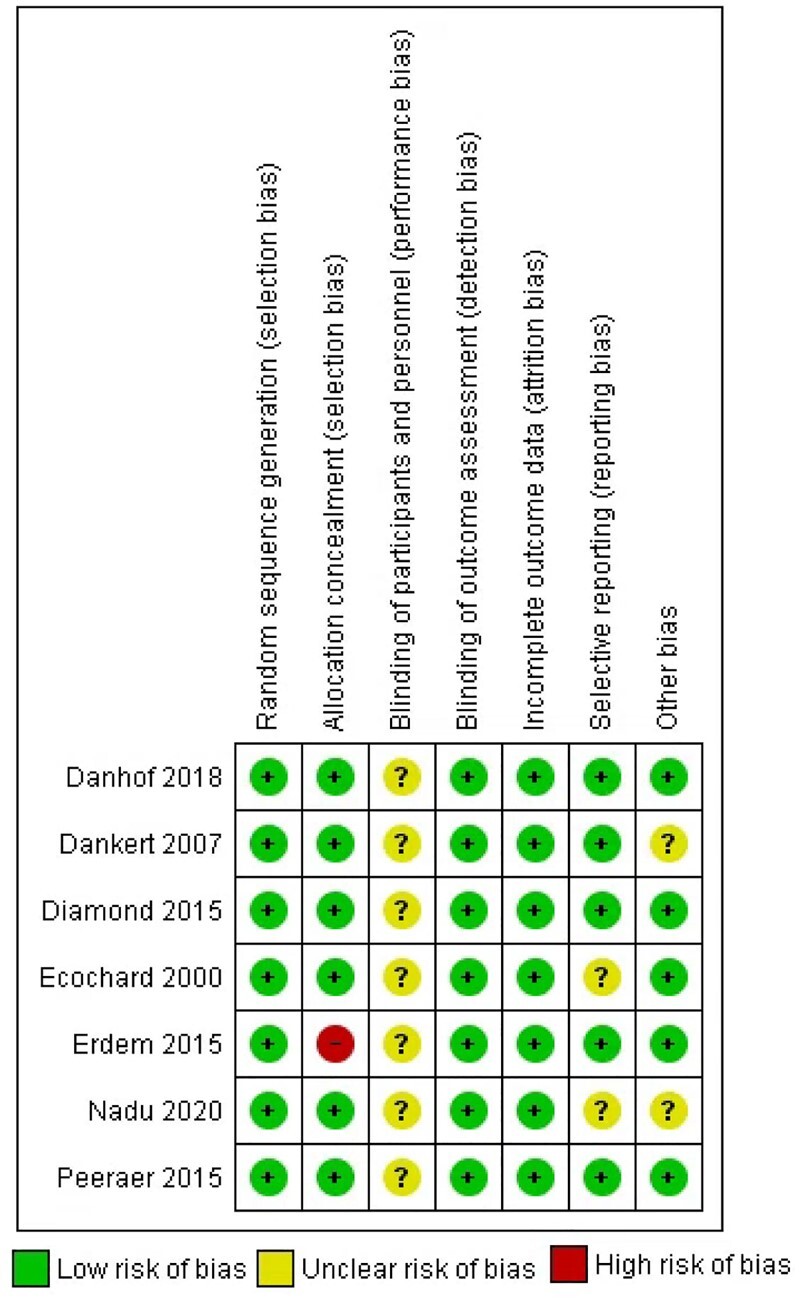
We searched electronic databases including MEDLINE, EMBASE, CENTRAL, CINAHL, and PsycINFO from their inception to 28 June 2021. We included randomized controlled trials (RCTs) comparing IUI-OS with gonadotrophins, letrozole and CC among couples with unexplained infertility. We contacted the authors of eligible RCTs to share the IPD and established the IUI IPD-MA Collaboration. The primary effectiveness outcome was live birth and the primary safety outcome was multiple pregnancy. Secondary outcomes were other reproductive outcomes, including time to conception leading to live birth. We performed a one-stage random effects IPD-MA.
Seven of 22 (31.8%) eligible RCTs provided IPD of 2495 couples (62.4% of the 3997 couples participating in 22 RCTs), of which 2411 had unexplained infertility and were included in this IPD-MA. Six RCTs (n = 1511) compared gonadotrophins with CC, and one (n = 900) compared gonadotrophins, letrozole and CC. Moderate-certainty evidence showed that gonadotrophins increased the live birth rate compared to CC (6 RCTs, 2058 women, RR 1.30, 95% CI 1.12-1.51, I2 = 26%). Low-certainty evidence showed that gonadotrophins may also increase the multiple pregnancy rate compared to CC (6 RCTs, 2058 women, RR 2.17, 95% CI 1.33-3.54, I2 = 69%). Heterogeneity on multiple pregnancy could be explained by differences in gonadotrophin starting dose and choice of cancellation criteria. Post-hoc sensitivity analysis on RCTs with a low starting dose of gonadotrophins (≤75 IU) confirmed increased live birth rates compared to CC (5 RCTs, 1457 women, RR 1.26, 95% CI 1.05-1.51), but analysis on only RCTs with stricter cancellation criteria showed inconclusive evidence on live birth (4 RCTs, 1238 women, RR 1.15, 95% CI 0.94-1.41). For multiple pregnancy, both sensitivity analyses showed inconclusive findings between gonadotrophins and CC (RR 0.94, 95% CI 0.45-1.96; RR 0.81, 95% CI 0.32-2.03, respectively). Moderate certainty evidence showed that gonadotrophins reduced the time to conception leading to a live birth when compared to CC (6 RCTs, 2058 women, HR 1.37, 95% CI 1.15-1.63, I2 = 22%). No strong evidence on the treatment-covariate (female age, BMI or primary versus secondary infertility) interactions was found.
In couples with unexplained infertility undergoing IUI-OS, gonadotrophins increased the chance of a live birth and reduced the time to conception compared to CC, at the cost of a higher multiple pregnancy rate, when not differentiating strategies on cancellation criteria or the starting dose. The treatment effects did not seem to differ in women of different age, BMI or primary versus secondary infertility. In a modern practice where a lower starting dose and stricter cancellation criteria are in place, effectiveness and safety of different agents seem both acceptable, and therefore intervention availability, cost and patients' preferences should factor in the clinical decision-making. As the evidence for comparisons to letrozole is based on one RCT providing IPD, further RCTs comparing letrozole and other interventions for unexplained infertility are needed.
宫腔内人工授精联合卵巢刺激(IUI-OS)是不明原因不孕的一线治疗方法。促性腺激素、来曲唑和枸橼酸氯米酚(CC)是 IUI-OS 期间常用的药物,已在多项汇总数据荟萃分析中进行了比较,这些分析存在大量异质性,且没有对时间至事件结局进行分析。个体参与者数据荟萃分析(IPD-MA)被认为是证据综合的金标准,因为它可以通过获取 IPD 来弥补个别研究报告不足的问题,并允许对治疗-协变量相互作用进行分析,以确定哪些夫妇从特定治疗中获益最大。
我们进行了这项 IPD-MA,以比较促性腺激素、来曲唑和 CC 用于刺激卵巢的有效性和安全性,并探索在接受 IUI 的夫妇中,重要基线特征的治疗-协变量相互作用。
我们检索了包括 MEDLINE、EMBASE、CENTRAL、CINAHL 和 PsycINFO 在内的电子数据库,检索时间从数据库建立到 2021 年 6 月 28 日。我们纳入了比较 IUI-OS 与促性腺激素、来曲唑和 CC 治疗不明原因不孕夫妇的随机对照试验(RCT)。我们联系了合格 RCT 的作者,分享 IPD,并成立了 IUI IPD-MA 合作。主要有效性结局是活产,主要安全性结局是多胎妊娠。次要结局包括其他生殖结局,包括导致活产的受孕时间。我们进行了一项单阶段随机效应 IPD-MA。
22 项(31.8%)合格 RCT 中的 7 项(62.4%,即 3997 项 RCT 中有 2495 对夫妇)提供了 2411 对有不明原因不孕的夫妇的 IPD,这些夫妇被纳入了本次 IPD-MA。6 项 RCT(n=1511)比较了促性腺激素与 CC,1 项 RCT(n=900)比较了促性腺激素、来曲唑和 CC。中等确定性证据表明,与 CC 相比,促性腺激素增加了活产率(6 项 RCT,2058 名女性,RR 1.30,95%CI 1.12-1.51,I²=26%)。低确定性证据表明,与 CC 相比,促性腺激素可能也增加了多胎妊娠率(6 项 RCT,2058 名女性,RR 2.17,95%CI 1.33-3.54,I²=69%)。多胎妊娠的异质性可以通过促性腺激素起始剂量和取消标准的选择来解释。对促性腺激素起始剂量较低(≤75IU)的 RCT 的事后敏感性分析证实,与 CC 相比,活产率增加(5 项 RCT,1457 名女性,RR 1.26,95%CI 1.05-1.51),但仅对取消标准更严格的 RCT 进行分析显示,活产的证据不一致(4 项 RCT,1238 名女性,RR 1.15,95%CI 0.94-1.41)。对于多胎妊娠,两种敏感性分析均显示促性腺激素与 CC 之间的结果不一致(RR 0.94,95%CI 0.45-1.96;RR 0.81,95%CI 0.32-2.03)。中等确定性证据表明,与 CC 相比,促性腺激素降低了导致活产的受孕时间(6 项 RCT,2058 名女性,HR 1.37,95%CI 1.15-1.63,I²=22%)。没有发现治疗-协变量(女性年龄、BMI 或原发与继发不孕)相互作用的有力证据。
在接受 IUI-OS 的不明原因不孕夫妇中,与 CC 相比,促性腺激素增加了活产的机会,并缩短了受孕时间,但多胎妊娠率更高,而取消标准或起始剂量的策略没有差异。在年龄、BMI 或原发与继发不孕不同的女性中,治疗效果似乎没有差异。在现代实践中,使用较低的起始剂量和更严格的取消标准,不同药物的有效性和安全性似乎都可以接受,因此干预的可用性、成本和患者的偏好应该纳入临床决策。由于比较来曲唑的证据仅基于一项提供 IPD 的 RCT,因此需要进一步的 RCT 比较来曲唑和其他用于不明原因不孕的干预措施。