Department of Health Care Medicine, Kawasaki Medical School General Medical Center, 2-6-1, Nakasange, Kita-ku, Okayama, 700-8505, Japan.
Guidelines Committee for Creating and Evaluating the ''Evidence-Based Clinical Practice Guidelines for Peptic Ulcer," the Japanese Society of Gastroenterology (JSGE), 6F Shimbashi i-MARK Bldg., 2-6-2 Shimbashi, Minato-ku, Tokyo, 105-0004, Japan.
J Gastroenterol. 2021 Apr;56(4):303-322. doi: 10.1007/s00535-021-01769-0. Epub 2021 Feb 23.
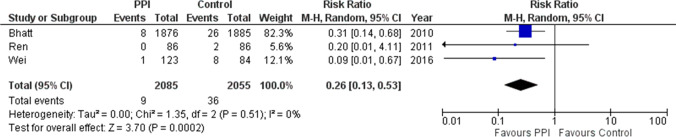
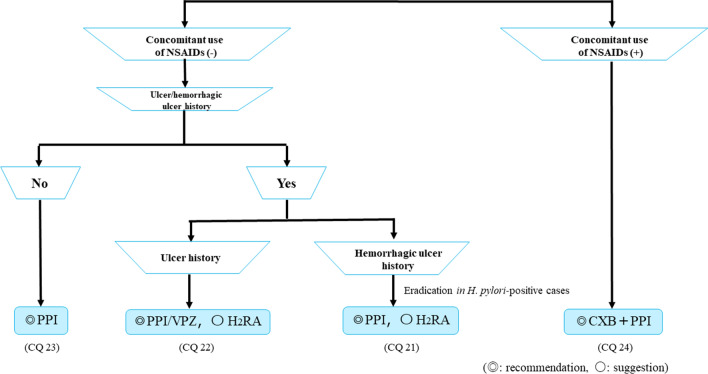
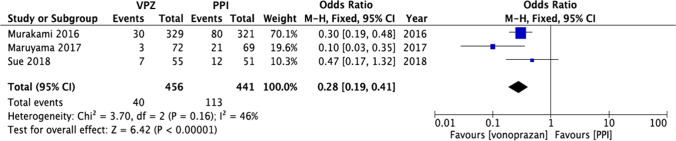
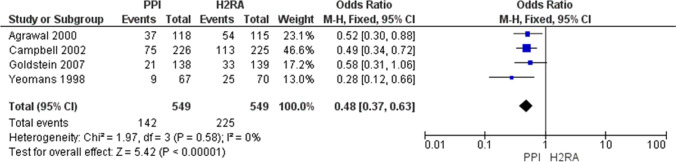
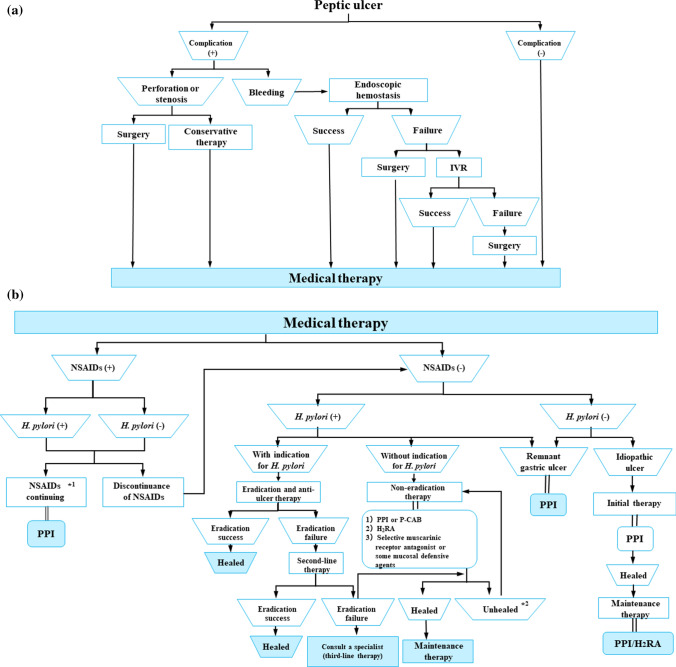
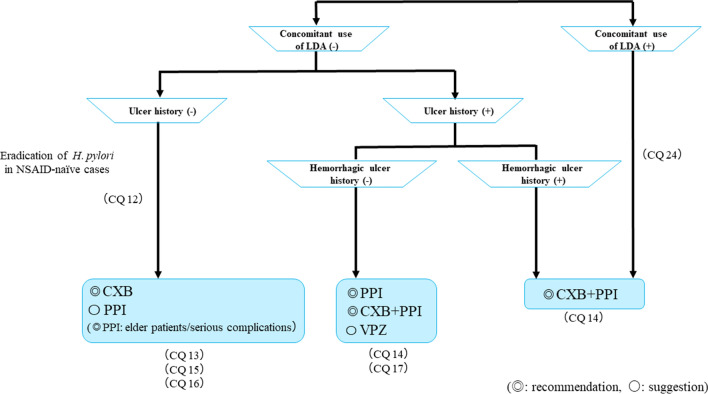
The Japanese Society of Gastroenterology (JSGE) revised the third edition of evidence-based clinical practice guidelines for peptic ulcer disease in 2020 and created an English version. The revised guidelines consist of nine items: epidemiology, hemorrhagic gastric and duodenal ulcers, Helicobacter pylori (H. pylori) eradication therapy, non-eradication therapy, drug-induced ulcers, non-H. pylori, and nonsteroidal anti-inflammatory drug (NSAID) ulcers, remnant gastric ulcers, surgical treatment, and conservative therapy for perforation and stenosis. Therapeutic algorithms for the treatment of peptic ulcers differ based on ulcer complications. In patients with NSAID-induced ulcers, NSAIDs are discontinued and anti-ulcer therapy is administered. If NSAIDs cannot be discontinued, the ulcer is treated with proton pump inhibitors (PPIs). Vonoprazan (VPZ) with antibiotics is recommended as the first-line treatment for H. pylori eradication, and PPIs or VPZ with antibiotics is recommended as a second-line therapy. Patients who do not use NSAIDs and are H. pylori negative are considered to have idiopathic peptic ulcers. Algorithms for the prevention of NSAID- and low-dose aspirin (LDA)-related ulcers are presented in this guideline. These algorithms differ based on the concomitant use of LDA or NSAIDs and ulcer history or hemorrhagic ulcer history. In patients with a history of ulcers receiving NSAID therapy, PPIs with or without celecoxib are recommended and the administration of VPZ is suggested for the prevention of ulcer recurrence. In patients with a history of ulcers receiving LDA therapy, PPIs or VPZ are recommended and the administration of a histamine 2-receptor antagonist is suggested for the prevention of ulcer recurrence.
日本胃肠病学会(JSGE)于 2020 年修订了第三版《消化性溃疡病循证临床实践指南》,并制作了英文版本。修订后的指南包括九个项目:流行病学、胃和十二指肠出血性溃疡、幽门螺杆菌(H. pylori)根除治疗、非根除治疗、药物性溃疡、非 H. pylori 和非甾体抗炎药(NSAID)溃疡、残胃溃疡、手术治疗以及穿孔和狭窄的保守治疗。消化性溃疡的治疗算法因溃疡并发症而异。对于 NSAID 诱导性溃疡患者,应停止使用 NSAIDs 并给予抗溃疡治疗。如果不能停用 NSAIDs,则用质子泵抑制剂(PPIs)治疗溃疡。抗生素联合 vonoprazan(VPZ)被推荐作为 H. pylori 根除的一线治疗药物,PPIs 或 VPZ 联合抗生素被推荐作为二线治疗药物。不使用 NSAIDs 且 H. pylori 阴性的患者被认为患有特发性消化性溃疡。本指南提出了 NSAID 和低剂量阿司匹林(LDA)相关溃疡预防的算法。这些算法根据同时使用 LDA 或 NSAIDs 以及溃疡史或出血性溃疡史而有所不同。对于正在接受 NSAID 治疗且有溃疡史的患者,建议使用 PPI 联合或不联合塞来昔布,建议使用 VPZ 预防溃疡复发。对于正在接受 LDA 治疗且有溃疡史的患者,建议使用 PPI 或 VPZ,并建议使用组胺 2 受体拮抗剂预防溃疡复发。