Tehranian Shahrzad, Shawwa Khaled, Kashani Kianoush B
Department of Medicine, Division of Nephrology and Hypertension, Mayo Clinic, Rochester, MN, USA.
Department of Medicine, Division of Pulmonary and Critical Care Medicine, Mayo Clinic, Rochester, MN, USA.
Clin Kidney J. 2019 Dec 17;14(2):564-569. doi: 10.1093/ckj/sfz179. eCollection 2021 Feb.
Fluid overload, a critical consequence of acute kidney injury (AKI), is associated with worse outcomes. The optimal fluid removal rate per day during continuous renal replacement therapy (CRRT) is unknown. The purpose of this study is to evaluate the impact of the ultrafiltration rate on mortality in critically ill patients with AKI receiving CRRT.
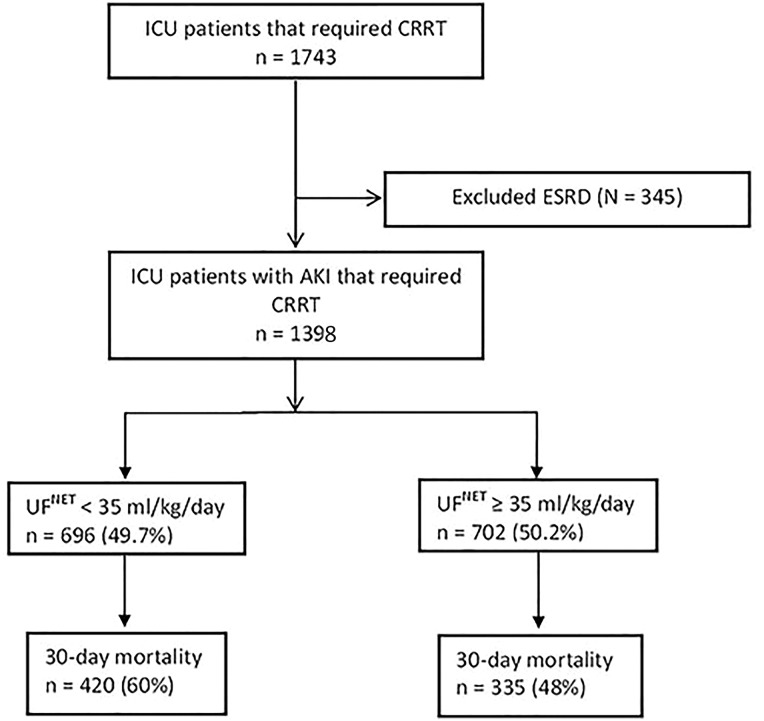
This was a retrospective cohort study where we reviewed 1398 patients with AKI who received CRRT between December 2006 and November 2015 at the Mayo Clinic, Rochester, MN, USA. The net ultrafiltration rate (UF) was categorized into low- and high-intensity groups (<35 and ≥35 mL/kg/day, respectively). The impact of different UF intensities on 30-day mortality was assessed using logistic regression after adjusting for age, sex, body mass index, fluid balance from intensive care unit (ICU) admission to CRRT initiation, Acute Physiologic Assessment and Chronic Health Evaluation III and sequential organ failure assessment scores, baseline serum creatinine, ICU day at CRRT initiation, Charlson comorbidity index, CRRT duration and need of mechanical ventilation.
The mean ± SD age was 62 ± 15 years, and 827 (59%) were male. There were 696 patients (49.7%) in the low- and 702 (50.2%) in the high-intensity group. Thirty-day mortality was 755 (54%). There were 420 (60%) deaths in the low-, and 335 (48%) in the high-intensity group (P < 0.001). UF ≥35 mL/kg/day remained independently associated with lower 30-day mortality (adjusted odds ratio = 0.47, 95% confidence interval 0.37-0.59; P < 0.001) compared with <35 mL/kg/day.
More intensive fluid removal, UF ≥35 mL/kg/day, among AKI patients receiving CRRT is associated with lower mortality. Future prospective studies are required to confirm this finding.
液体超负荷是急性肾损伤(AKI)的一个关键后果,与更差的预后相关。连续性肾脏替代治疗(CRRT)期间的最佳每日液体清除率尚不清楚。本研究的目的是评估超滤率对接受CRRT的AKI危重症患者死亡率的影响。
这是一项回顾性队列研究,我们回顾了2006年12月至2015年11月在美国明尼苏达州罗切斯特市梅奥诊所接受CRRT的1398例AKI患者。净超滤率(UF)被分为低强度和高强度组(分别为<35和≥35 mL/kg/天)。在调整年龄、性别、体重指数、从重症监护病房(ICU)入院到开始CRRT的液体平衡、急性生理评估和慢性健康评估III以及序贯器官衰竭评估评分、基线血清肌酐、开始CRRT时的ICU天数、Charlson合并症指数、CRRT持续时间和机械通气需求后,使用逻辑回归评估不同UF强度对30天死亡率的影响。
平均年龄±标准差为62±15岁,男性827例(59%)。低强度组有696例患者(49.7%),高强度组有702例患者(50.2%)。30天死亡率为755例(54%)。低强度组有420例(60%)死亡,高强度组有335例(48%)死亡(P<0.001)。与<35 mL/kg/天相比,UF≥35 mL/kg/天仍然独立地与较低的30天死亡率相关(调整后的优势比=0.47,95%置信区间0.37-0.59;P<0.001)。
在接受CRRT的AKI患者中,更强化的液体清除,即UF≥35 mL/kg/天,与较低的死亡率相关。需要未来的前瞻性研究来证实这一发现。