Centre for Health Informatics, Health Data Research UK North, School of Health Sciences, Faculty of Biology, Medicine, and Health, the University of Manchester, Manchester, UK.
Public Health England North West, Manchester, UK.
Clin Infect Dis. 2021 Nov 16;73(10):1805-1812. doi: 10.1093/cid/ciab159.
Antimicrobial resistance is a serious global health concern that emphasizes completing treatment course. Recently, the effectiveness of short versus longer antibiotic courses has been questioned. This study investigated the duration of prescribed antibiotics, their effectiveness, and associated risk of infection-related complications.
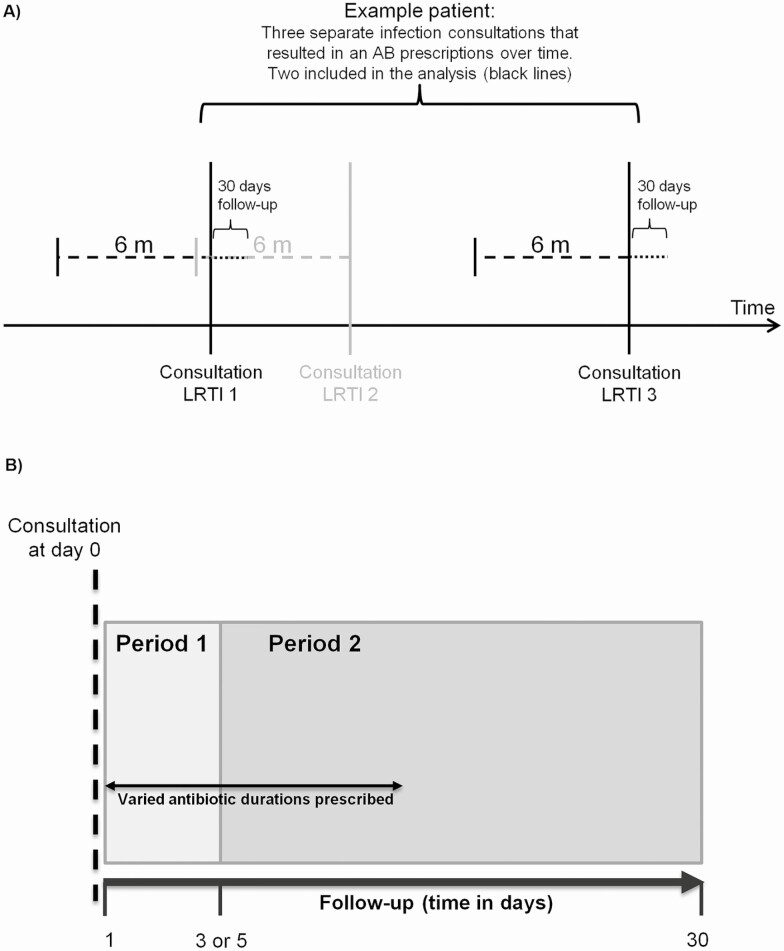
Clinical Practice Research Datalink identified 4 million acute infection episodes prescribed an antibiotic in primary care between January 2014-June 2014, England. Prescriptions were categorized by duration. Risk of infection-related hospitalizations within 30 days was modelled overall and by infection type. Risk was assessed immediately after or within 30 days follow-up to measure confounders given similar and varying exposure, respectively. An interaction term with follow-up time assessed whether hazard ratios (HRs) remained parallel with different antibiotic durations.
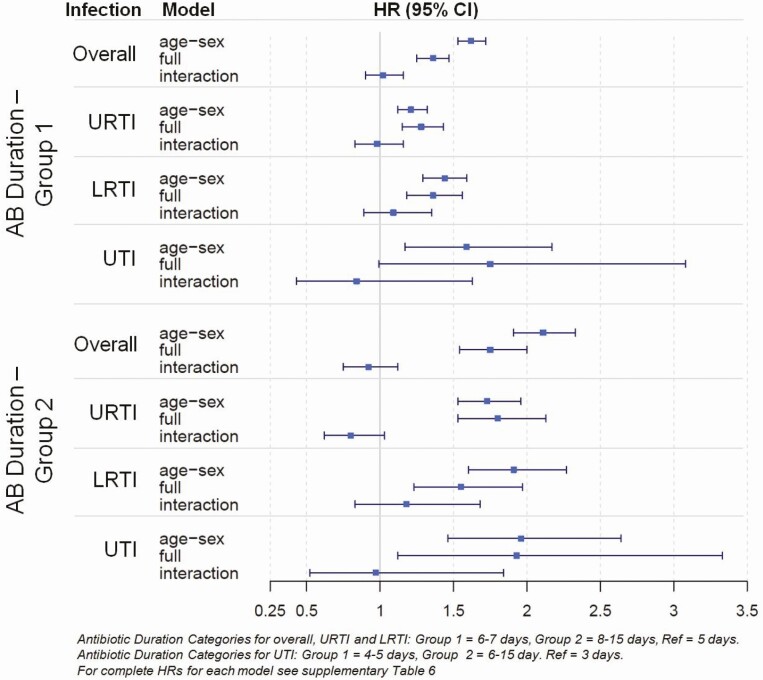
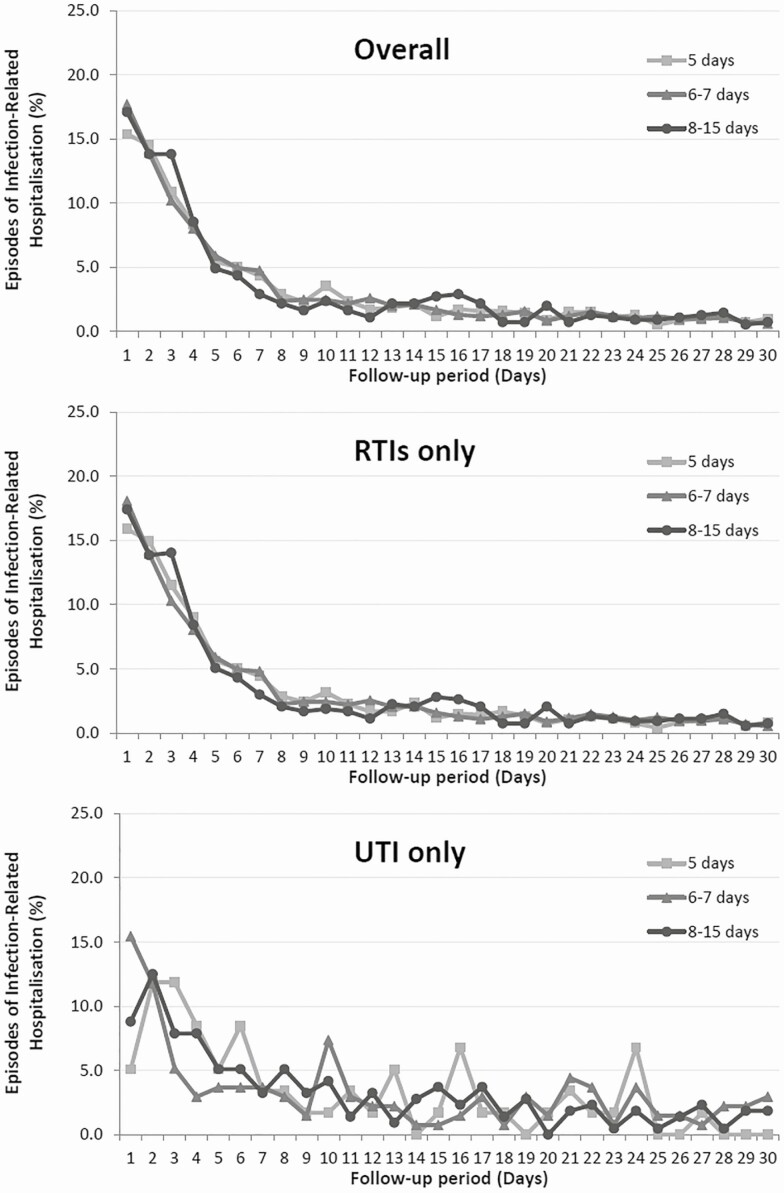
The duration of antibiotic courses increased over the study period (5.2-19.1%); 6-7 days were most common (66.9%). Most infection-related hospitalizations occurred with prescriptions of 8-15 days (0.21%), accompanied by greater risk of infection-related complications compared to patients who received a short prescription (HR: 1.75 [95% CI: 1.54-2.00]). Comparing HRs in the first 5 days versus remaining follow-up showed longer antibiotic courses were no more effective than shorter courses (1.02 [95% CI: 0.90-1.16] and 0.92 [95% CI: 0.75-1.12]). No variation by infection-type was observed.
Equal effectiveness was found between shorter and longer antibiotic courses and the reduction of infection-related hospitalizations. Stewardship programs should recommend shorter courses of antibiotics for acute infections. Further research is required for treating patients with a complex medical history.SummaryPrescribing of longer courses increased over the study period. The majority of hospitalizations occurred for patients receiving longer courses. Risk of developing a complication (immediate vs remaining follow-up) found longer courses were no more effective than shorter courses.
抗菌药物耐药性是一个严重的全球健康问题,强调完成治疗疗程。最近,人们对短疗程与长疗程抗生素的疗效产生了质疑。本研究调查了处方抗生素的持续时间、疗效以及与感染相关并发症的风险。
临床实践研究数据链(Clinical Practice Research Datalink)于 2014 年 1 月至 2014 年 6 月期间在初级保健中确定了 400 万例急性感染病例,这些病例均接受了抗生素治疗。处方的持续时间按类别分类。在总体和按感染类型对 30 天内感染相关住院的风险进行建模。风险评估是在立即或 30 天随访后进行的,以分别衡量相似和不同暴露下的混杂因素。与随访时间的交互项评估了危险比(HRs)是否与不同的抗生素持续时间保持平行。
研究期间抗生素疗程的持续时间增加(5.2-19.1%);6-7 天最常见(66.9%)。大多数感染相关的住院治疗发生在使用 8-15 天处方的患者中(0.21%),与接受短期处方的患者相比,这些患者感染相关并发症的风险更高(HR:1.75 [95% CI:1.54-2.00])。比较前 5 天与剩余随访的 HR 表明,较长的抗生素疗程并不比较短的疗程更有效(1.02 [95% CI:0.90-1.16] 和 0.92 [95% CI:0.75-1.12])。未观察到感染类型的差异。
发现较短和较长疗程的抗生素疗效相等,感染相关住院治疗减少。管理方案应为急性感染推荐较短疗程的抗生素。需要进一步研究为治疗有复杂病史的患者提供依据。总结:研究期间,较长疗程的处方增加。大多数住院患者接受了较长疗程的治疗。(立即 vs 剩余随访)发现并发症风险更长的疗程并不比更短的疗程更有效。