The Cleveland Clinic Foundation Cleveland OH.
University of Alabama Birmingham AL.
J Am Heart Assoc. 2021 Feb;10(5):e017619. doi: 10.1161/JAHA.120.017619. Epub 2021 Feb 25.
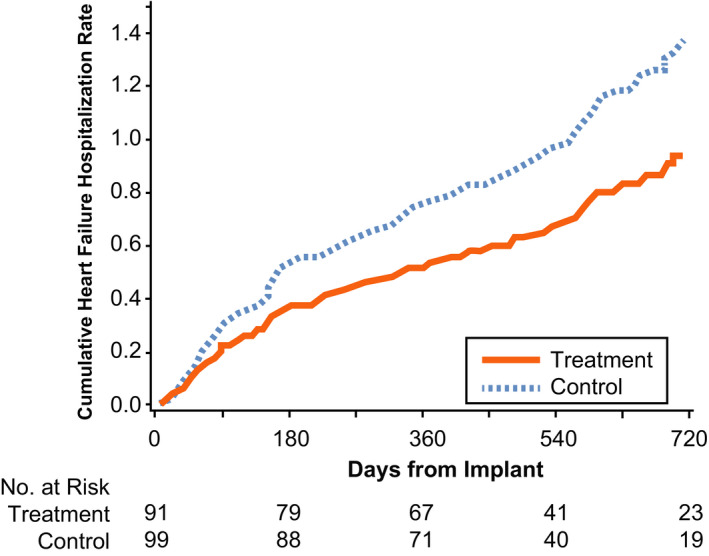
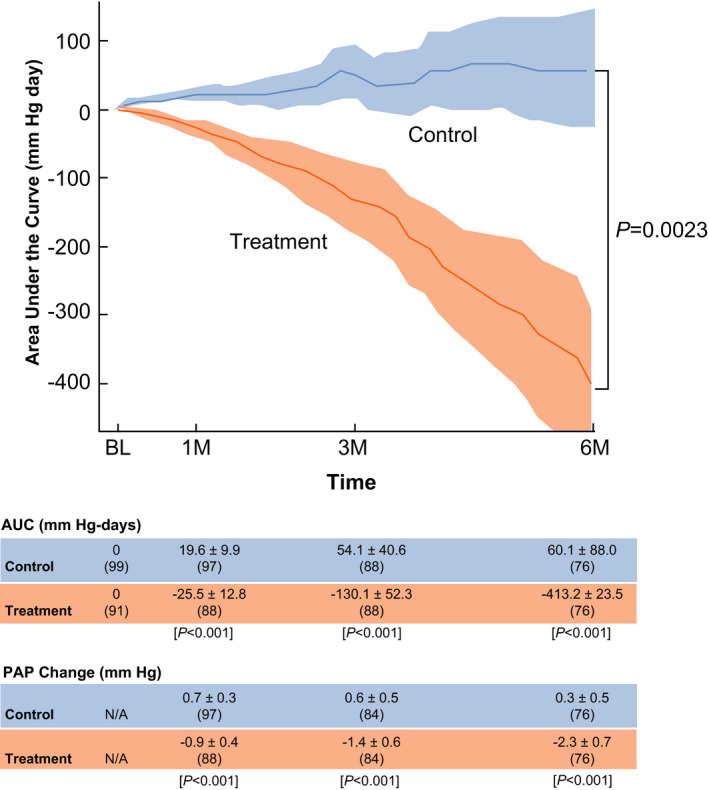
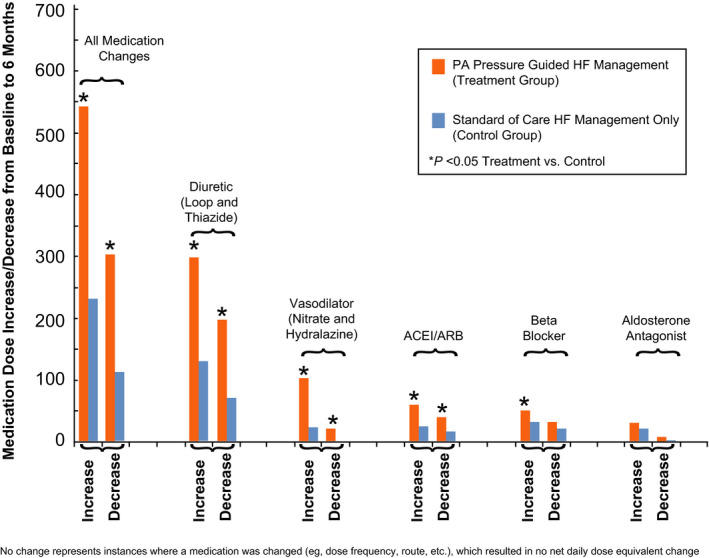
Background Patients with recurring heart failure (HF) following cardiac resynchronization therapy fare poorly. Their management is undecided. We tested remote hemodynamic-guided pharmacotherapy. Methods and Results We evaluated cardiac resynchronization therapy subjects included in the CHAMPION (CardioMEMS Heart Sensor Allows Monitoring of Pressure to Improve Outcomes in New York Heart Association Class III Heart Failure Patients) trial, which randomized patients with persistent New York Heart Association Class III symptoms and ≥1 HF hospitalization in the previous 12 months to remotely managed pulmonary artery (PA) pressure-guided management (treatment) or usual HF care (control). Diuretics and/or vasodilators were adjusted conventionally in control and included remote PA pressure information in treatment. Annualized HF hospitalization rates, changes in PA pressures over time (analyzed by area under the curve), changes in medications, and quality of life (Minnesota Living with Heart Failure Questionnaire scores) were assessed. Patients who had cardiac resynchronization therapy (n=190, median implant duration 755 days) at enrollment had poor hemodynamic function (cardiac index 2.00±0.59 L/min per m), high comorbidity burden (67% had secondary pulmonary hypertension, 61% had estimated glomerular filtration rate <60 mL/min per 1.73 m), and poor Minnesota Living with Heart Failure Questionnaire scores (57±24). During 18 months randomized follow-up, HF hospitalizations were 30% lower in treatment (n=91, 62 events, 0.46 events/patient-year) versus control patients (n=99, 93 events, 0.68 events/patient-year) (hazard ratio, 0.70; 95% CI, 0.51-0.96; =0.028). Treatment patients had more medication up-/down-titrations (847 versus 346 in control, <0.001), mean PA pressure reduction (area under the curve -413.2±123.5 versus 60.1±88.0 in control, =0.002), and quality of life improvement (Minnesota Living with Heart Failure Questionnaire decreased -13.5±23 versus -4.9±24.8 in control, =0.006). Conclusions Remote hemodynamic-guided adjustment of medical therapies decreased PA pressures and the burden of HF symptoms and hospitalizations in patients with recurring Class III HF and hospitalizations, beyond the effect of cardiac resynchronization therapy. Registration URL: https://www.clinicaltrials.gov; Unique identifier: NCT00531661.
心脏再同步治疗后反复发作心力衰竭(HF)的患者预后较差。他们的治疗方案尚未确定。我们测试了远程血流动力学指导的药物治疗。
我们评估了 CHAMPION(CardioMEMS 心脏传感器允许监测压力以改善纽约心脏协会 III 类心力衰竭患者的预后)试验中纳入的心脏再同步治疗患者,该试验将 12 个月内持续存在纽约心脏协会 III 类症状和≥1 次 HF 住院的患者随机分为远程管理肺动脉(PA)压力指导管理(治疗)或常规 HF 护理(对照)。对照组常规调整利尿剂和/或血管扩张剂,并包括治疗中的远程 PA 压力信息。评估了 HF 住院的年度发生率、随时间变化的 PA 压力变化(通过曲线下面积分析)、药物变化和生活质量(明尼苏达州心力衰竭生活质量问卷评分)。入组时接受心脏再同步治疗的患者(n=190,中位植入时间 755 天)血流动力学功能较差(心指数 2.00±0.59 L/min/每 m),合并症负担较重(67%患有继发性肺动脉高压,61%估计肾小球滤过率<60 ml/min/每 1.73 m),明尼苏达州心力衰竭生活质量问卷评分较低(57±24)。在 18 个月的随机随访期间,治疗组(n=91,62 例事件,0.46 例/患者年)HF 住院率较对照组(n=99,93 例事件,0.68 例/患者年)降低 30%(风险比,0.70;95%置信区间,0.51-0.96;=0.028)。治疗组的药物剂量调整更为频繁(治疗组 847 次,对照组 346 次,<0.001),平均 PA 压力降低(曲线下面积-413.2±123.5 与对照组 60.1±88.0,=0.002),生活质量改善(明尼苏达州心力衰竭生活质量问卷评分降低-13.5±23 与对照组-4.9±24.8,=0.006)。
远程血流动力学指导的药物治疗调整可降低反复发作 III 类 HF 患者的 PA 压力和 HF 症状及住院负担,并超过心脏再同步治疗的效果。