Department of Preclinical Pharmacology, R&D, Chiesi Farmaceutici S.P.A., 43122, Parma, Italy.
Scientific Consultant, 48640, Bilbao, Spain.
Respir Res. 2021 Feb 26;22(1):71. doi: 10.1186/s12931-020-01585-9.
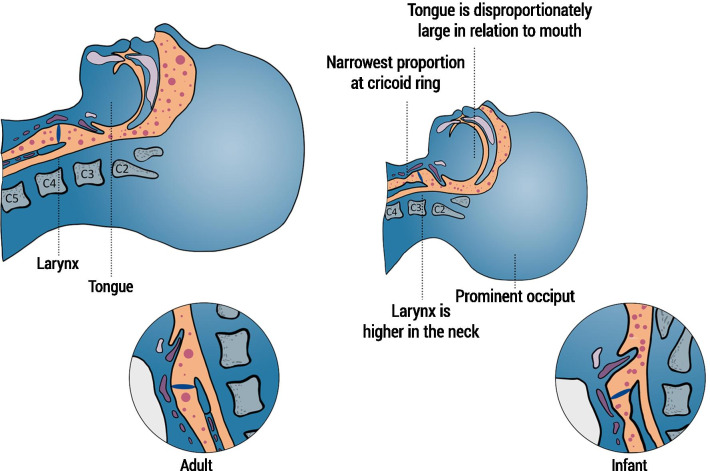
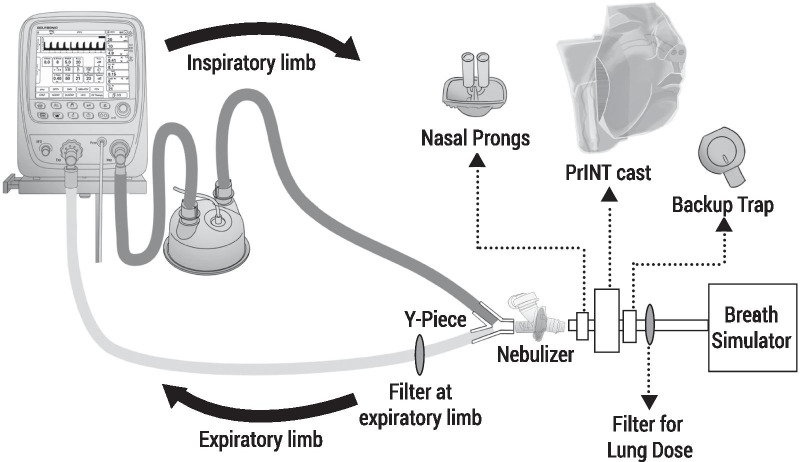
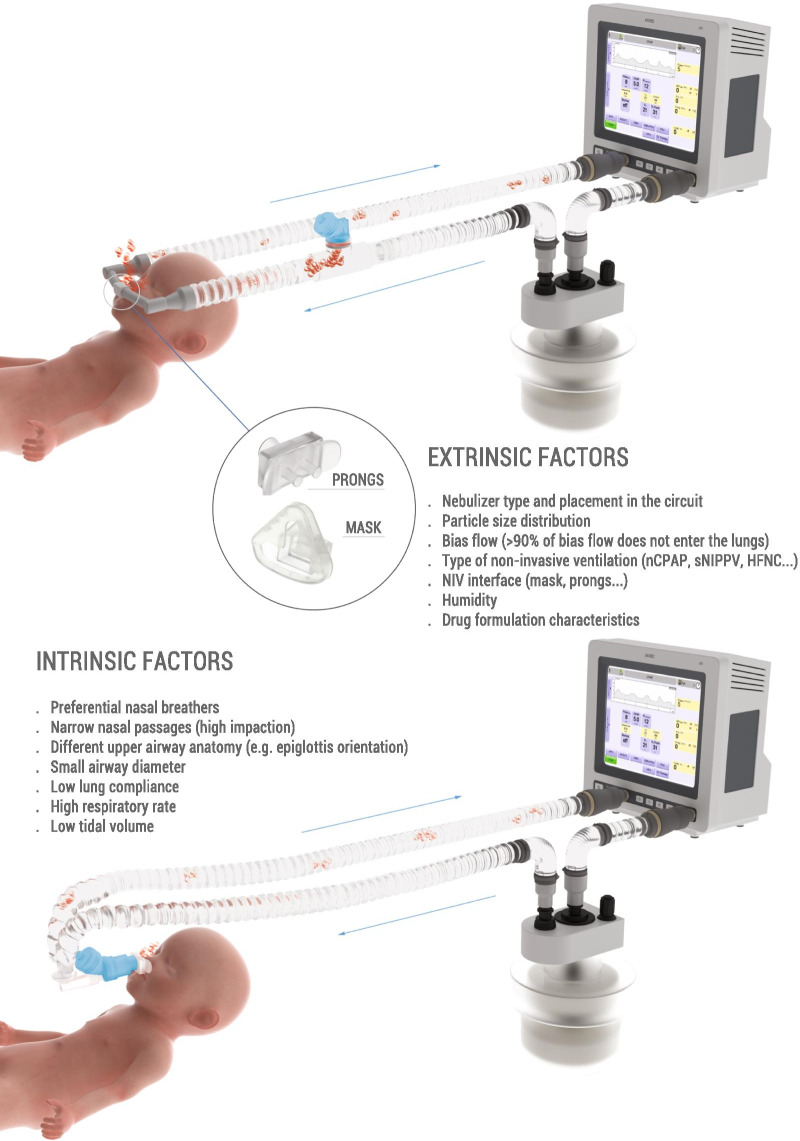
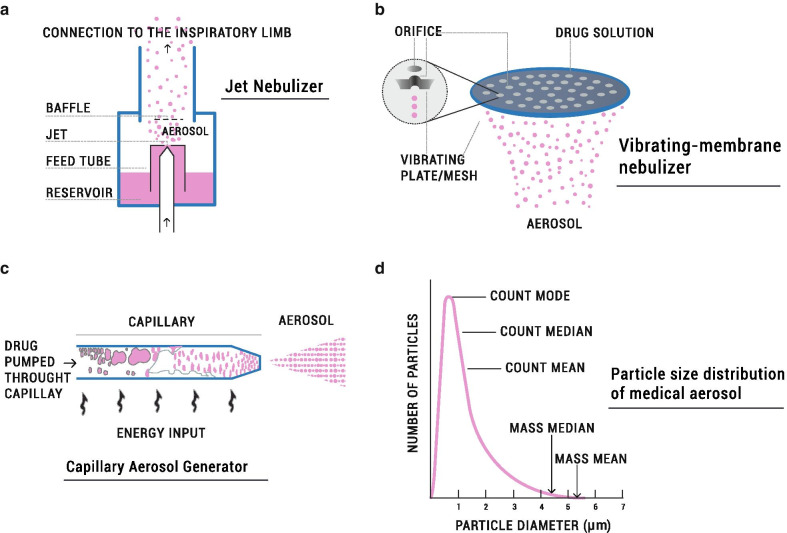
Delivery of medications to preterm neonates receiving non-invasive ventilation (NIV) represents one of the most challenging scenarios for aerosol medicine. This challenge is highlighted by the undersized anatomy and the complex (patho)physiological characteristics of the lungs in such infants. Key physiological restraints include low lung volumes, low compliance, and irregular respiratory rates, which significantly reduce lung deposition. Such factors are inherent to premature birth and thus can be regarded to as the intrinsic factors that affect lung deposition. However, there are a number of extrinsic factors that also impact lung deposition: such factors include the choice of aerosol generator and its configuration within the ventilation circuit, the drug formulation, the aerosol particle size distribution, the choice of NIV type, and the patient interface between the delivery system and the patient. Together, these extrinsic factors provide an opportunity to optimize the lung deposition of therapeutic aerosols and, ultimately, the efficacy of the therapy.In this review, we first provide a comprehensive characterization of both the intrinsic and extrinsic factors affecting lung deposition in premature infants, followed by a revision of the clinical attempts to deliver therapeutic aerosols to premature neonates during NIV, which are almost exclusively related to the non-invasive delivery of surfactant aerosols. In this review, we provide clues to the interpretation of existing experimental and clinical data on neonatal aerosol delivery and we also describe a frame of measurable variables and available tools, including in vitro and in vivo models, that should be considered when developing a drug for inhalation in this important but under-served patient population.
将药物递送给接受无创通气 (NIV) 的早产儿是气溶胶药物治疗中最具挑战性的情况之一。这种挑战突出表现在婴儿的解剖结构较小,肺部的复杂(病理)生理特征上。关键的生理限制包括低肺容量、低顺应性和不规则的呼吸频率,这些都会显著降低肺部沉积。这些因素是早产儿出生所固有的,因此可以被视为影响肺部沉积的内在因素。然而,还有许多外在因素也会影响肺部沉积:这些因素包括气溶胶发生器的选择及其在通气回路中的配置、药物制剂、气溶胶粒径分布、NIV 类型的选择以及输送系统与患者之间的患者接口。这些外在因素共同为优化治疗性气溶胶的肺部沉积提供了机会,并最终提高治疗效果。
在这篇综述中,我们首先全面描述了影响早产儿肺部沉积的内在和外在因素,然后回顾了在 NIV 期间向早产儿输送治疗性气溶胶的临床尝试,这些尝试几乎都与表面活性剂气溶胶的无创输送有关。在这篇综述中,我们提供了对新生儿气溶胶输送现有实验和临床数据的解释线索,还描述了一个可衡量变量和可用工具的框架,包括体外和体内模型,当为这个重要但服务不足的患者群体开发吸入药物时,应考虑这些变量和工具。