Department of Cardiology, Aarhus University Hospital, Palle Juul-Jensens Boulevard 99, 8200, Aarhus N, Denmark.
Diagnostic Centre, Region Hospital of Silkeborg, Silkeborg, Denmark.
BMC Pulm Med. 2021 Feb 28;21(1):72. doi: 10.1186/s12890-021-01440-7.
To investigate if acute pulmonary vasodilation by sildenafil improves right ventricular function in patients with acute intermediate-high risk pulmonary embolism (PE).
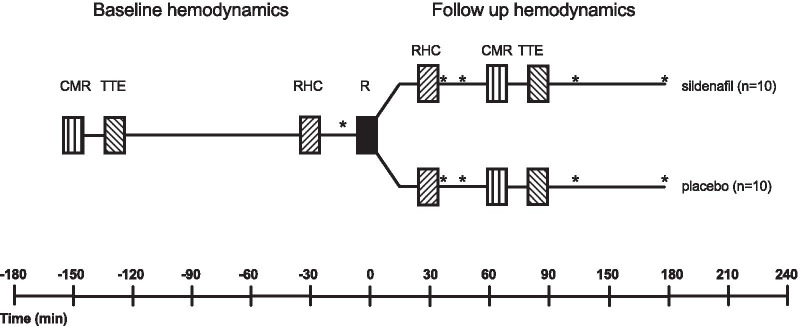
Single center, explorative trial. Patients with PE were randomized to a single oral dose of sildenafil 50 mg (n = 10) or placebo (n = 10) as add-on to conventional therapy. The time from hospital admission to study inclusion was 2.3 ± 0.7 days. Right ventricular function was evaluated immediately before and shortly after (0.5-1.5 h) randomization by right heart catheterization (RHC), trans-thoracic echocardiography (TTE), and cardiac magnetic resonance (CMR). The primary efficacy endpoint was cardiac index measured by CMR.
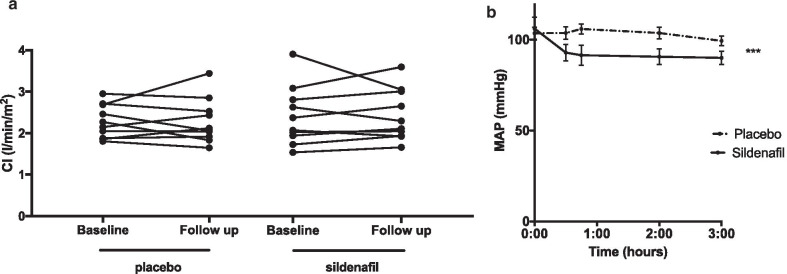
Patients had acute intermediate-high risk PE verified by computed tomography pulmonary angiography, systolic blood pressure of 135 ± 18 (mean ± SD) mmHg, increased right ventricular/left ventricular ratio 1.1 ± 0.09 and increased troponin T 167 ± 144 ng/L. Sildenafil treatment did not improve cardiac index compared to baseline (0.02 ± 0.36 l/min/m2, p = 0.89) and neither did placebo (0.00 ± 0.34 l/min/m2, p = 0.97). Sildenafil lowered mean arterial blood pressure (- 19 ± 10 mmHg, p < 0.001) which was not observed in the placebo group (0 ± 9 mmHg, p = 0.97).
A single oral dose of sildenafil 50 mg did not improve cardiac index but lowered systemic blood pressure in patients with acute intermediate-high risk PE. The time from PE to intervention, a small patient sample size and low pulmonary vascular resistance are limitations of this study that should be considered when interpreting the results.
The trial was retrospectively registered at www.clinicaltrials.gov (NCT04283240) February 2nd 2020, https://clinicaltrials.gov/ct2/show/NCT04283240?term=NCT04283240&draw=2&rank=1 .
研究在急性中高危肺栓塞(PE)患者中,西地那非的急性肺血管扩张是否改善右心室功能。
单中心、探索性试验。将 PE 患者随机分为口服单剂量西地那非 50mg(n=10)或安慰剂(n=10)作为常规治疗的附加治疗。从住院到纳入研究的时间为 2.3±0.7 天。通过右心导管检查(RHC)、经胸超声心动图(TTE)和心脏磁共振(CMR)在随机分组前即刻和短时间后(0.5-1.5 小时)评估右心室功能。主要疗效终点是 CMR 测量的心指数。
患者通过计算机断层扫描肺动脉造影证实为急性中高危 PE,收缩压为 135±18(均值±标准差)mmHg,右心室/左心室比值增加 1.1±0.09,肌钙蛋白 T 增加 167±144ng/L。与基线相比,西地那非治疗并未改善心指数(0.02±0.36l/min/m2,p=0.89),安慰剂也未改善心指数(0.00±0.34l/min/m2,p=0.97)。西地那非降低平均动脉血压(-19±10mmHg,p<0.001),而安慰剂组则无此现象(0±9mmHg,p=0.97)。
在急性中高危 PE 患者中,单次口服 50mg 西地那非不能改善心指数,但可降低全身血压。从 PE 到干预的时间、患者样本量小以及低肺血管阻力是本研究的局限性,在解释结果时应考虑这些因素。
该试验于 2020 年 2 月 2 日在 www.clinicaltrials.gov(NCT04283240)进行了回顾性注册,网址为 https://clinicaltrials.gov/ct2/show/NCT04283240?term=NCT04283240&draw=2&rank=1。