Lyhne Mads Dam, Kline Jeffrey Allen, Nielsen-Kudsk Jens Erik, Andersen Asger
Department of Cardiology, Aarhus University Hospital and Institute of Clinical Medicine, Aarhus University, Aarhus, Denmark.
Department of Emergency Medicine, Indiana University School of Medicine, Indianapolis, IN, USA.
Pulm Circ. 2020 Mar 4;10(1):2045894019899775. doi: 10.1177/2045894019899775. eCollection 2020 Jan-Mar.
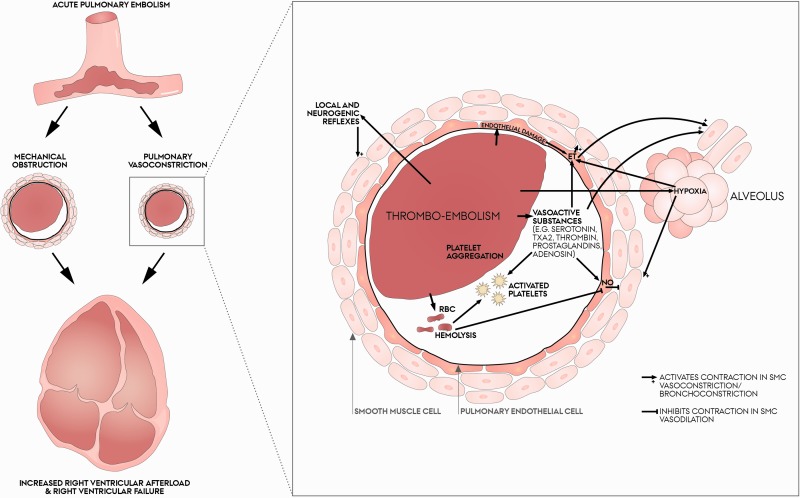
Acute pulmonary embolism is the third most common cause of cardiovascular death. Pulmonary embolism increases right ventricular afterload, which causes right ventricular failure, circulatory collapse and death. Most treatments focus on removal of the mechanical obstruction caused by the embolism, but pulmonary vasoconstriction is a significant contributor to the increased right ventricular afterload and is often left untreated. Pulmonary thromboembolism causes mechanical obstruction of the pulmonary vasculature coupled with a complex interaction between humoral factors from the activated platelets, endothelial effects, reflexes and hypoxia to cause pulmonary vasoconstriction that worsens right ventricular afterload. Vasoconstrictors include serotonin, thromboxane, prostaglandins and endothelins, counterbalanced by vasodilators such as nitric oxide and prostacyclins. Exogenous administration of pulmonary vasodilators in acute pulmonary embolism seems attractive but all come with a risk of systemic vasodilation or worsening of pulmonary ventilation-perfusion mismatch. In animal models of acute pulmonary embolism, modulators of the nitric oxide-cyclic guanosine monophosphate-protein kinase G pathway, endothelin pathway and prostaglandin pathway have been investigated. But only a small number of clinical case reports and prospective clinical trials exist. The aim of this review is to give an overview of the causes of pulmonary embolism-induced pulmonary vasoconstriction and of experimental and human investigations of pulmonary vasodilation in acute pulmonary embolism.
急性肺栓塞是心血管死亡的第三大常见原因。肺栓塞会增加右心室后负荷,进而导致右心室衰竭、循环衰竭和死亡。大多数治疗方法侧重于消除栓塞所致的机械性梗阻,但肺血管收缩是右心室后负荷增加的一个重要因素,且常常未得到治疗。肺血栓栓塞导致肺血管系统的机械性梗阻,同时激活的血小板产生的体液因子、内皮效应、反射和缺氧之间存在复杂的相互作用,从而引起肺血管收缩,使右心室后负荷加重。血管收缩剂包括5-羟色胺、血栓素、前列腺素和内皮素,而血管舒张剂如一氧化氮和前列环素则起到平衡作用。在急性肺栓塞中,外源性给予肺血管舒张剂似乎很有吸引力,但都存在全身血管舒张或肺通气-灌注不匹配恶化的风险。在急性肺栓塞的动物模型中,已经对一氧化氮-环磷酸鸟苷-蛋白激酶G途径、内皮素途径和前列腺素途径的调节剂进行了研究。但仅有少数临床病例报告和前瞻性临床试验。本综述的目的是概述肺栓塞引起肺血管收缩的原因以及急性肺栓塞中肺血管舒张的实验和人体研究情况。