Department of Oncology, University of Turin, Turin, Italy.
Departments of Pathology, University Healthy Network and University of Toronto, Toronto, Canada.
Endocr Pathol. 2021 Mar;32(1):154-168. doi: 10.1007/s12022-021-09668-z. Epub 2021 Feb 27.
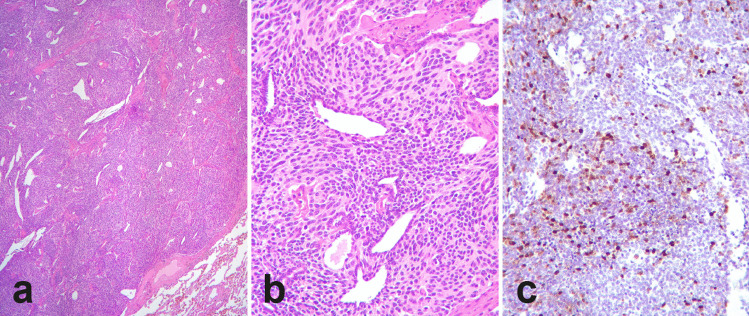
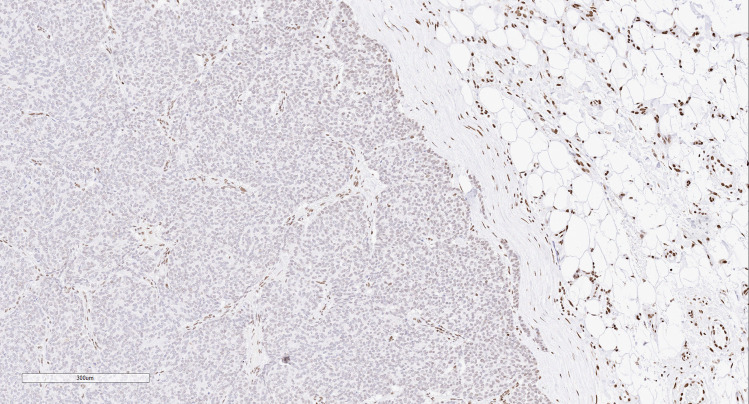
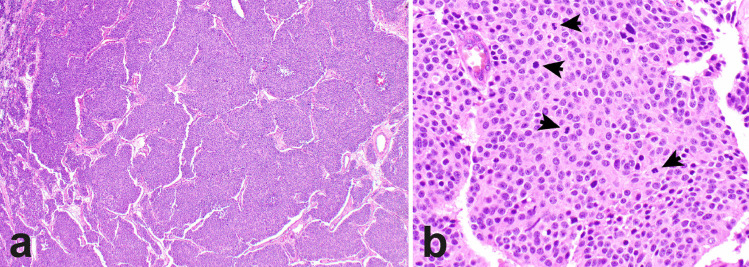
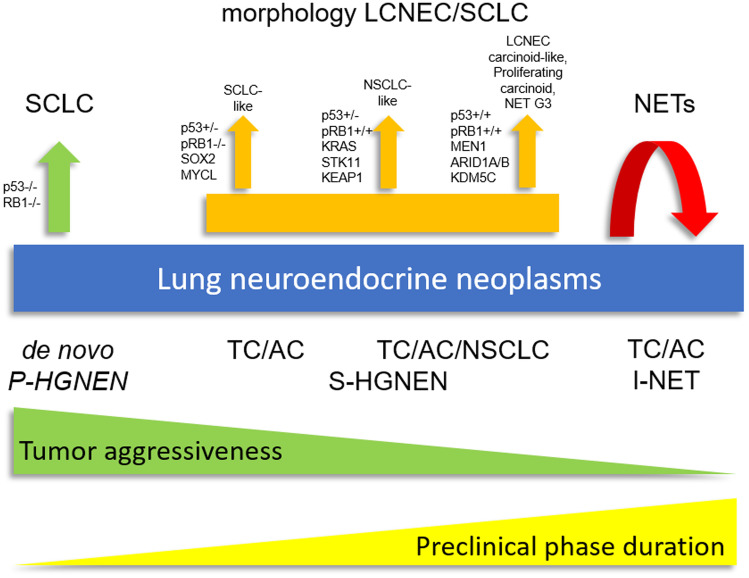
Thoracic (pulmonary and thymic) neuroendocrine tumors are well-differentiated epithelial neuroendocrine neoplasms that are classified into typical and atypical carcinoid tumors based on mitotic index cut offs and presence or absence of necrosis. This classification scheme is of great prognostic value but designed for surgical specimens, only. Deep molecular characterization of thoracic neuroendocrine tumors highlighted their difference with neuroendocrine carcinomas. Neuroendocrine tumors of the lung are characterized by a low mutational burden, and a high prevalence of mutations in chromatin remodeling and histone modification-related genes, whereas mutations in genes frequently altered in neuroendocrine carcinomas are rare. Molecular profiling divided thymic neuroendocrine tumors into three clusters with distinct clinical outcomes and characterized by a different average of copy number instability. Moreover, integrated histopathological, molecular and clinical evidence supports the existence of a grey zone category between neuroendocrine tumors (carcinoid tumors) and neuroendocrine carcinomas. Indeed, cases with well differentiated morphology but mitotic/Ki-67 indexes close to neuroendocrine carcinomas have been increasingly recognized. These are characterized by specific molecular profiles and have an aggressive clinical behavior. Finally, thoracic neuroendocrine tumors may arise in the background of genetic susceptibility, being MEN1 syndrome the well-defined familial form. However, pathologists should be aware of rarer germline variants that are associated with the concurrence of neuroendocrine tumors of the lung or their precursors (such as DIPNECH) with other neoplasms, including but not limited to breast carcinomas. Therefore, genetic counseling for all young patients with thoracic neuroendocrine neoplasia and/or any patient with pathological evidence of neuroendocrine cell hyperplasia-to-neoplasia progression sequence or multifocal disease should be considered.
胸部(肺和胸腺)神经内分泌肿瘤是分化良好的上皮神经内分泌肿瘤,根据有丝分裂指数的截止值和坏死的存在与否,分为典型和非典型类癌肿瘤。这种分类方案具有重要的预后价值,但仅适用于手术标本。对胸部神经内分泌肿瘤的深入分子特征分析突出了它们与神经内分泌癌的不同。肺神经内分泌肿瘤的特点是突变负担低,染色质重塑和组蛋白修饰相关基因的突变率高,而在神经内分泌癌中经常改变的基因的突变则很少。分子分析将胸腺癌分为三个簇,具有不同的临床结局,并具有不同的平均拷贝数不稳定性。此外,综合组织病理学、分子和临床证据支持神经内分泌肿瘤(类癌肿瘤)和神经内分泌癌之间存在一个灰色区域类别。事实上,具有良好分化形态但有丝分裂/ki-67 指数接近神经内分泌癌的病例越来越受到关注。这些病例具有特定的分子特征,具有侵袭性的临床行为。最后,胸部神经内分泌肿瘤可能在遗传易感性的背景下发生,MEN1 综合征是明确的家族形式。然而,病理学家应该意识到罕见的种系变异,这些变异与肺神经内分泌肿瘤或其前体(如 DIPNECH)与其他肿瘤的同时发生有关,包括但不限于乳腺癌。因此,应考虑对所有患有胸部神经内分泌肿瘤和/或任何有神经内分泌细胞增生-肿瘤进展序列或多灶性疾病病理证据的患者进行遗传咨询。