Ren Tai, Li Yong-Sheng, Dang Xue-Yi, Li Yang, Shao Zi-Yu, Bao Run-Fa, Shu Yi-Jun, Wang Xu-An, Wu Wen-Guang, Wu Xiang-Song, Li Mao-Lan, Cao Hong, Wang Kun-Hua, Cai Hong-Yu, Jin Chong, Jin Hui-Han, Yang Bo, Jiang Xiao-Qing, Gu Jian-Feng, Cui Yun-Fu, Zhang Zai-Yang, Zhu Chun-Fu, Sun Bei, Dai Chao-Liu, Zheng Lin-Hui, Cao Jing-Yu, Fei Zhe-Wei, Liu Chang-Jun, Li Bing, Liu Jun, Qian Ye-Ben, Wang Yi, Hua Ya-Wei, Zhang Xi, Liu Chang, Lau Wan-Yee, Liu Ying-Bin
Department of General Surgery, Xinhua Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai 200092, China.
Shanghai Key Laboratory of Biliary Tract Disease Research, Shanghai 200092, China.
World J Gastrointest Surg. 2021 Feb 27;13(2):176-186. doi: 10.4240/wjgs.v13.i2.176.
Whether regional lymphadenectomy (RL) should be routinely performed in patients with T1b gallbladder cancer (GBC) remains a subject of debate.
To investigate whether RL can improve the prognosis of patients with T1b GBC.
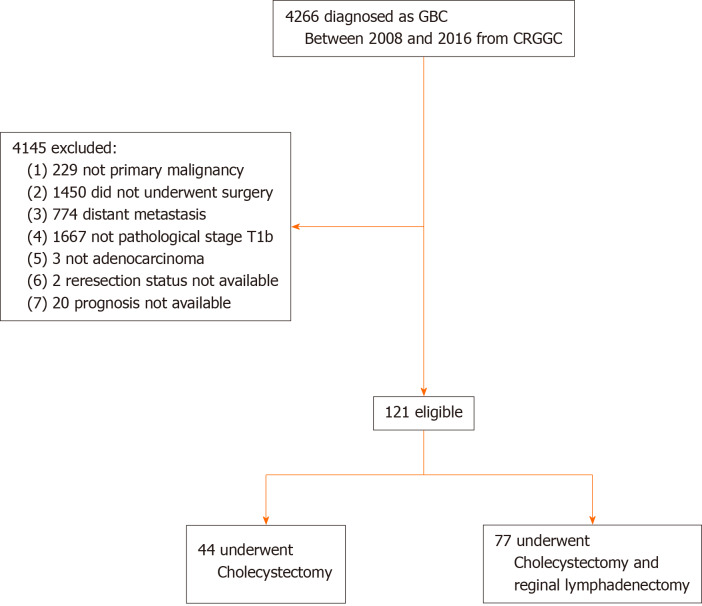
We studied a multicenter cohort of patients with T1b GBC who underwent surgery between 2008 and 2016 at 24 hospitals in 13 provinces in China. The log-rank test and Cox proportional hazards model were used to compare the overall survival (OS) of patients who underwent cholecystectomy (Ch) + RL and those who underwent Ch only. To investigate whether combined hepatectomy (Hep) improved OS in T1b patients, we studied patients who underwent Ch + RL to compare the OS of patients who underwent combined Hep and patients who did not.
Of the 121 patients (aged 61.9 ± 10.1 years), 77 (63.6%) underwent Ch + RL, and 44 (36.4%) underwent Ch only. Seven (9.1%) patients in the Ch + RL group had lymph node metastasis. The 5-year OS rate was significantly higher in the Ch + RL group than in the Ch group (76.3% 56.8%, = 0.036). Multivariate analysis showed that Ch + RL was significantly associated with improved OS (hazard ratio: 0.51; 95% confidence interval: 0.26-0.99). Among the 77 patients who underwent Ch + RL, no survival improvement was found in patients who underwent combined Hep (5-year OS rate: 79.5% for combined Hep and 76.1% for no Hep; = 0.50).
T1b GBC patients who underwent Ch + RL had a better prognosis than those who underwent Ch. Hep + Ch showed no improvement in prognosis in T1b GBC patients. Although recommended by both the National Comprehensive Cancer Network and Chinese Medical Association guidelines, RL was only performed in 63.6% of T1b GBC patients. Routine Ch + RL should be advised in T1b GBC.
对于T1b期胆囊癌(GBC)患者是否应常规进行区域淋巴结清扫术(RL)仍存在争议。
探讨RL是否能改善T1b期GBC患者的预后。
我们研究了2008年至2016年期间在中国13个省份的24家医院接受手术的T1b期GBC患者的多中心队列。采用对数秩检验和Cox比例风险模型比较接受胆囊切除术(Ch)+RL的患者与仅接受Ch的患者的总生存期(OS)。为了研究联合肝切除术(Hep)是否能改善T1b期患者的OS,我们研究了接受Ch+RL的患者,比较接受联合Hep的患者与未接受联合Hep的患者的OS。
121例患者(年龄61.9±10.1岁)中,77例(63.6%)接受了Ch+RL,44例(36.4%)仅接受了Ch。Ch+RL组中有7例(9.1%)患者发生淋巴结转移。Ch+RL组的5年OS率显著高于Ch组(76.3%对56.8%,P=0.036)。多因素分析显示,Ch+RL与OS改善显著相关(风险比:0.51;95%置信区间:0.26-0.99)。在77例接受Ch+RL的患者中,接受联合Hep的患者未发现生存期改善(联合Hep的5年OS率:79.5%,未接受联合Hep的为76.1%;P=0.50)。
接受Ch+RL的T1b期GBC患者的预后优于仅接受Ch的患者。Hep+Ch在T1b期GBC患者中未显示出预后改善。尽管美国国立综合癌症网络和中国医学协会指南均推荐,但RL仅在63.6%的T1b期GBC患者中进行。对于T1b期GBC,建议常规进行Ch+RL。