Department of Public Health, Erasmus MC, University Medical Center Rotterdam, Rotterdam, The Netherlands.
Department of Gastroenterology & Hepatology, Erasmus MC, University Medical Center Rotterdam, Rotterdam, The Netherlands.
Int J Cancer. 2021 Jul 15;149(2):337-346. doi: 10.1002/ijc.33540. Epub 2021 Mar 25.
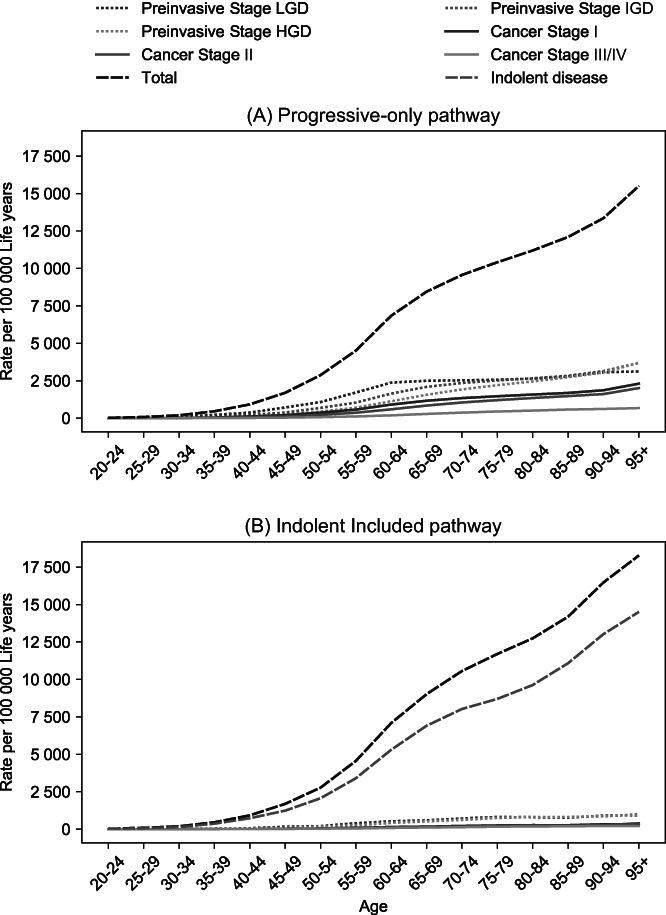
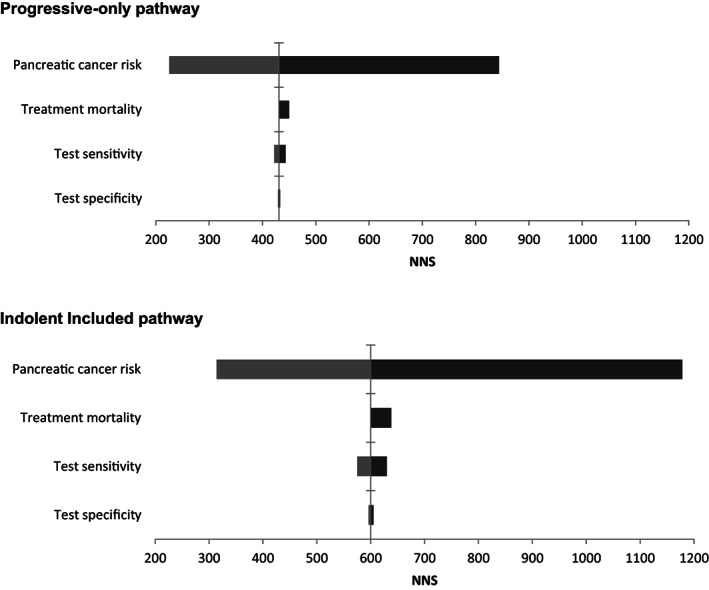
Pancreatic cancer (PC) survival is poor, as detection usually occurs late, when treatment options are limited. Screening of high-risk individuals may enable early detection and a more favorable prognosis. Knowledge gaps prohibit establishing the effectiveness of screening. We developed a Microsimulation Screening Analysis model to analyze the impact of relevant uncertainties on the effect of PC screening in high-risk individuals. The model simulates two base cases: one in which lesions always progress to PC and one in which indolent and faster progressive lesions coexist. For each base case, the effect of annual and 5-yearly screening with endoscopic ultrasonography/magnetic resonance imaging was evaluated. The impact of variance in PC risk, screening test characteristics and surgery-related mortality was evaluated using sensitivity analyses. Screening resulted in a reduction of PC mortality by at least 16% in all simulated scenarios. This reduction depended strongly on the natural disease course (annual screening: -57% for "Progressive-only" vs -41% for "Indolent Included"). The number of screen and surveillance tests needed to prevent one cancer death was impacted most by PC risk. A 10% increase in test sensitivity reduced mortality by 1.9% at most. Test specificity is important for the number of surveillance tests. In conclusion, screening reduces PC mortality in all modeled scenarios. The natural disease course and PC risk strongly determines the effectiveness of screening. Test sensitivity seems of lesser influence than specificity. Future research should gain more insight in PC pathobiology to establish the true value of PC screening in high-risk individuals.
胰腺癌(PC)的生存率很低,因为通常在治疗选择有限时才被检测到,而此时已经很晚了。对高危人群进行筛查可能有助于早期发现并获得更好的预后。由于知识上的差距,目前尚无法确定筛查的有效性。我们开发了一种微模拟筛查分析模型,以分析相关不确定性对高危人群中 PC 筛查效果的影响。该模型模拟了两种基本情况:一种是病变总是进展为 PC,另一种是惰性和快速进展性病变共存。对于每种基本情况,我们评估了每年和每 5 年进行内镜超声检查/磁共振成像筛查的效果。通过敏感性分析评估了 PC 风险、筛查试验特征和与手术相关的死亡率的变化的影响。在所有模拟场景中,筛查均使 PC 死亡率至少降低了 16%。这种减少在很大程度上取决于自然疾病过程(每年筛查:“仅进展型”为-57%,“惰性包含型”为-41%)。预防一例癌症死亡所需的筛查和监测测试数量受 PC 风险的影响最大。检测灵敏度提高 10%,死亡率最多降低 1.9%。检测特异性对监测测试的数量很重要。总之,在所有模拟场景中,筛查都降低了 PC 死亡率。自然疾病过程和 PC 风险强烈决定了筛查的效果。检测灵敏度的影响似乎不如特异性重要。未来的研究应该更深入地了解 PC 的病理生物学,以确定高危人群中 PC 筛查的真正价值。