Pathology, Medicine Oncology, Johns Hopkins University, Baltimore, Maryland, USA
Gastroenterology and Hepatology, Erasmus University Medical Center, Rotterdam, The Netherlands.
Gut. 2020 Jan;69(1):7-17. doi: 10.1136/gutjnl-2019-319352. Epub 2019 Oct 31.
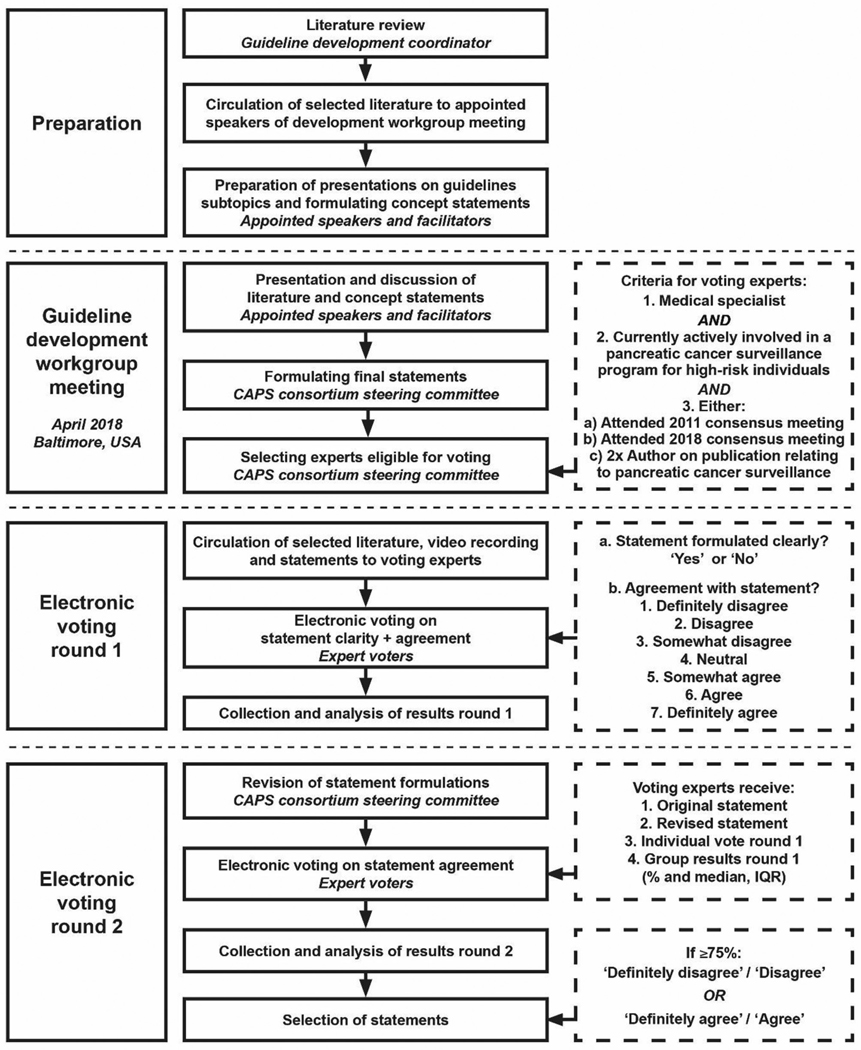
The International Cancer of the Pancreas Screening Consortium met in 2018 to update its consensus recommendations for the management of individuals with increased risk of pancreatic cancer based on family history or germline mutation status (high-risk individuals).
A modified Delphi approach was employed to reach consensus among a multidisciplinary group of experts who voted on consensus statements. Consensus was considered reached if ≥75% agreed or disagreed.
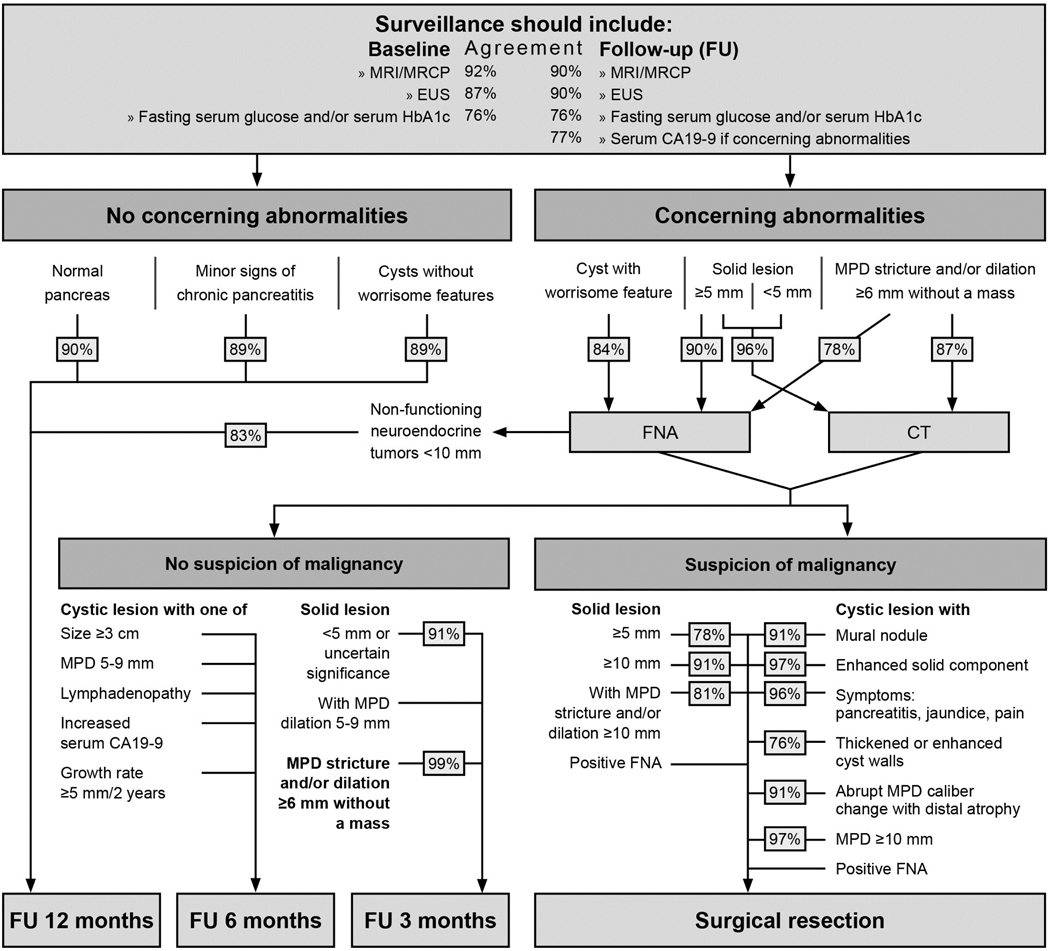
Consensus was reached on 55 statements. The main goals of surveillance (to identify high-grade dysplastic precursor lesions and T1N0M0 pancreatic cancer) remained unchanged. Experts agreed that for those with familial risk, surveillance should start no earlier than age 50 or 10 years earlier than the youngest relative with pancreatic cancer, but were split on whether to start at age 50 or 55. Germline mutation carriers with one affected first-degree relative are now considered eligible for surveillance. Experts agreed that preferred surveillance tests are endoscopic ultrasound and MRI/magnetic retrograde cholangiopancreatography, but no consensus was reached on how to alternate these modalities. Annual surveillance is recommended in the absence of concerning lesions. Main areas of disagreement included if and how surveillance should be performed for hereditary pancreatitis, and the management of indeterminate lesions.
Pancreatic surveillance is recommended for selected high-risk individuals to detect early pancreatic cancer and its high-grade precursors, but should be performed in a research setting by multidisciplinary teams in centres with appropriate expertise. Until more evidence supporting these recommendations is available, the benefits, risks and costs of surveillance of pancreatic surveillance need additional evaluation.
国际胰腺癌筛查联盟于 2018 年举行会议,根据家族史或种系突变状态(高危个体)更新了其关于管理具有胰腺癌风险增加个体的共识建议。
采用改良 Delphi 方法,让多学科专家小组对共识声明进行投票,以达成共识。如果≥75%的人同意或不同意,则达成共识。
就 55 项声明达成共识。监测的主要目标(识别高级别发育不良前体病变和 T1N0M0 胰腺癌)保持不变。专家们一致认为,对于有家族风险的人,监测应不早于 50 岁或比最年轻的胰腺癌亲属早 10 年开始,但对于从 50 岁还是 55 岁开始存在分歧。现在,携带一种致病性种系突变且有一位一级亲属受累的个体被认为有资格进行监测。专家们一致认为,首选的监测检查是内镜超声和 MRI/磁共振胰胆管成像,但如何交替使用这些方式尚未达成共识。在没有可疑病变的情况下,建议每年进行监测。主要的争议领域包括是否以及如何对遗传性胰腺炎进行监测,以及如何处理不确定的病变。
建议对选定的高危个体进行胰腺监测,以早期发现胰腺癌及其高级别前体病变,但应由多学科团队在具有适当专业知识的中心以研究为基础进行。在获得更多支持这些建议的证据之前,需要进一步评估胰腺监测的收益、风险和成本。