Iwasaki Masashi, Shimomura Masanori, Ii Tsunehiro
Department of General Thoracic Surgery, Ayabe City Hospital, 20-1 Otsuka, Aono-cho, Ayabe, Kyoto, 623-0011, Japan.
Division of Thoracic Surgery, Department of Surgery, Graduate School of Medical Science, Kyoto Prefectural University of Medicine, 465 Kajii-cho, Kawaramachi-Hirokoji, Kamigyo, Kyoto, 602-8566, Japan.
Surg Case Rep. 2021 Mar 2;7(1):61. doi: 10.1186/s40792-021-01144-4.
Bronchopleural fistula, which usually accompanies bronchial fistula and empyema, is a severe complication of lung cancer surgery. Negative-pressure wound therapy can enhance drainage and reduce the empyema cavity, potentially leading to early recovery. This therapy is not currently indicated for bronchopleural fistulas because of the risk of insufficient respiration due to air loss from the fistula.
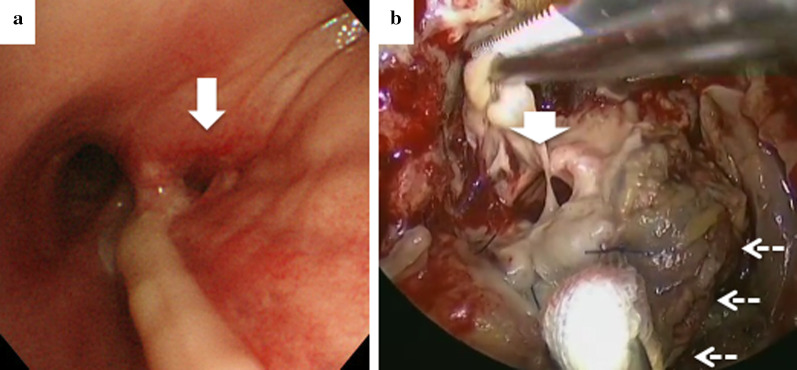
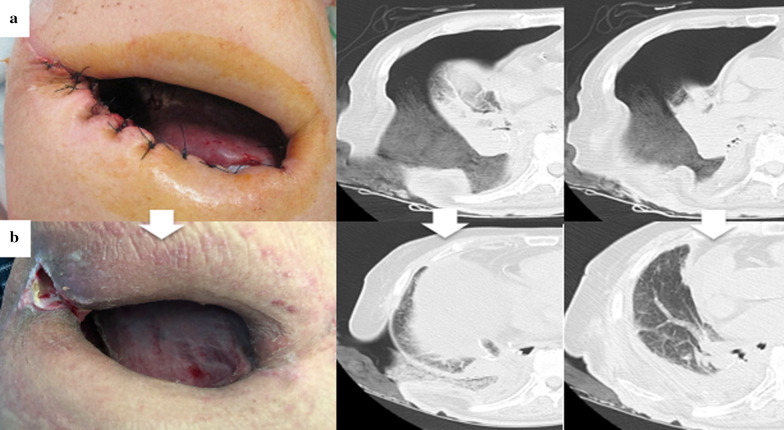
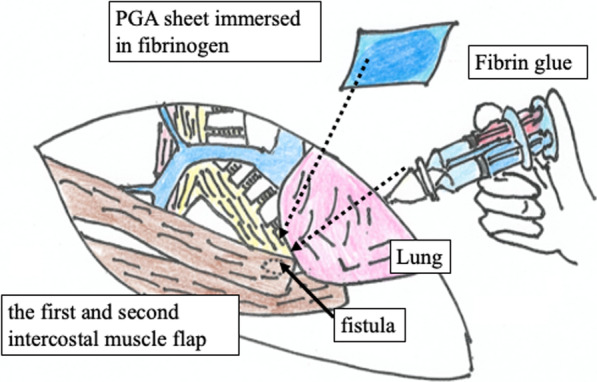
A 73-year-old man, who was malnourished because of peritoneal dialysis, was referred to our hospital for the treatment of lung cancer. Right lower lobectomy with mediastinal lymph node dissection was performed via posterolateral thoracotomy, and the bronchial stump was covered with the intercostal muscle flap. His postoperative course was uneventful and he was discharged. However, he was readmitted to our hospital because of respiratory failure and diagnosed as having bronchopleural fistula on the basis of the bronchoscopic finding of a 10-mm hole at the membranous portion of the inlet of the remnant lower lobe bronchus. Thus, thoracotomy debridement and open window thoracostomy were immediately performed. After achieving infection control, bronchial occlusion was performed using fibrin glue and a polyglycolic acid sheet was inserted through a fenestrated wound. Bronchial fistula closure was observed on bronchoscopy; therefore, a negative-pressure wound therapy system was applied to close the fenestrated wound. The collapsed lung was re-expanded and the granulation tissue around the wound increased; therefore, thoracic cavity size decreased and thoracoplasty using the latissimus dorsi was performed.
This bronchopleural fistula was treated successfully after a right lower lobectomy using an extra-pleural bronchial occlusion and negative-pressure wound therapy.
支气管胸膜瘘通常伴有支气管瘘和脓胸,是肺癌手术的严重并发症。负压伤口治疗可增强引流并减少脓胸腔,有可能促进早期康复。由于瘘口漏气有导致呼吸不足的风险,目前该疗法未被用于支气管胸膜瘘。
一名73岁男性,因腹膜透析导致营养不良,因肺癌治疗转诊至我院。通过后外侧开胸进行右下肺叶切除术及纵隔淋巴结清扫术,支气管残端用肋间肌瓣覆盖。术后恢复顺利,患者出院。然而,他因呼吸衰竭再次入院,根据支气管镜检查发现残留下叶支气管入口膜部有一个10毫米的洞,被诊断为支气管胸膜瘘。因此,立即进行了开胸清创和开窗胸廓造口术。在控制感染后,使用纤维蛋白胶进行支气管封堵,并通过有孔伤口插入聚乙醇酸片。支气管镜检查观察到支气管瘘闭合;因此,应用负压伤口治疗系统封闭有孔伤口。萎陷的肺重新扩张,伤口周围的肉芽组织增多;因此,胸腔尺寸减小,并采用背阔肌进行胸廓成形术。
该例支气管胸膜瘘在右下肺叶切除术后通过胸膜外支气管封堵和负压伤口治疗成功治愈。