Biondi Mia J, Garnett Lauren, Bello Alexander, Funk Duane, Poliquin Philippe Guillaume, Jones Shane, Tierney Kevin, Tran Kaylie, Kozak Robert A, Leung Anders, Grolla Allen, Nakamura Cory, Soule Geoff, Ranadheera Charlene, Hagan Mable, Dhaliwal Amrinder, Kobasa Darwyn, Falzarano Darryl, Bovendo Hugues Fausther, Feldmann Heinz, Kesselman Murray, Hansen Gregory, Gren Jason, Mortimer Todd, Racine Trina, Deschambault Yvon, Edmonds Jocelyn, Aminian Sam, Saurette Ray, Allan Mark, Rondeau Lauren, Huynh John, Hadder Sharron, Press Christy, DeGraff Christine, Kucas Stephanie, Kubay Julie, Azanarsky Kimberly, Cook Bradley W M, Hancock B J, Kumar Anand, Soni Reeni, Schantz Daryl, McKitrick Jarrid, Warner Bryce, Griffin Bryan D, Qiu Xiangguo, Kobinger Gary P, Safronetz Dave, Wood Heidi, R Stein Derek, Cutts Todd, Pickering Brad, Kenny James, Theriault Steven, Menec Liam, Vendramelli Robert, Higgins Sean, Banadyga Logan, Liu Guodong, Rahim Md Niaz, Kasloff Samantha, Sloan Angela, He Shihua, Tailor Nikesh, Albietz Alixandra, Wong Gary, Gray Michael, Feldmann Friederike, Marzi Andrea, Risi George, Strong James E
Toronto Centre for Liver Disease, University Health Network, Toronto, ON M5G 2C4, Canada.
National Microbiology Laboratory, Public Health Agency of Canada, Winnipeg, MB R3E 3M4, Canada.
Microorganisms. 2021 Feb 26;9(3):498. doi: 10.3390/microorganisms9030498.
The 2014-2016 Ebola outbreak in West Africa recapitulated that nosocomial spread of Ebola virus could occur and that health care workers were at particular risk including notable cases in Europe and North America. These instances highlighted the need for centers to better prepare for potential Ebola virus cases; including understanding how the virus spreads and which interventions pose the greatest risk.
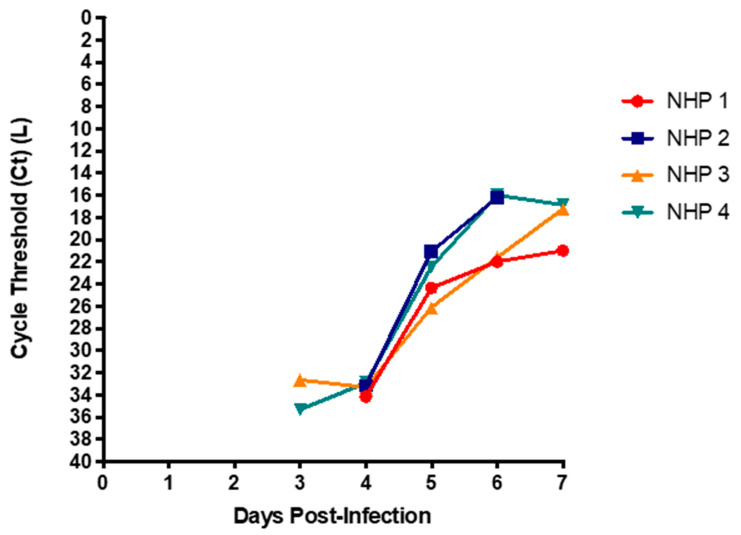
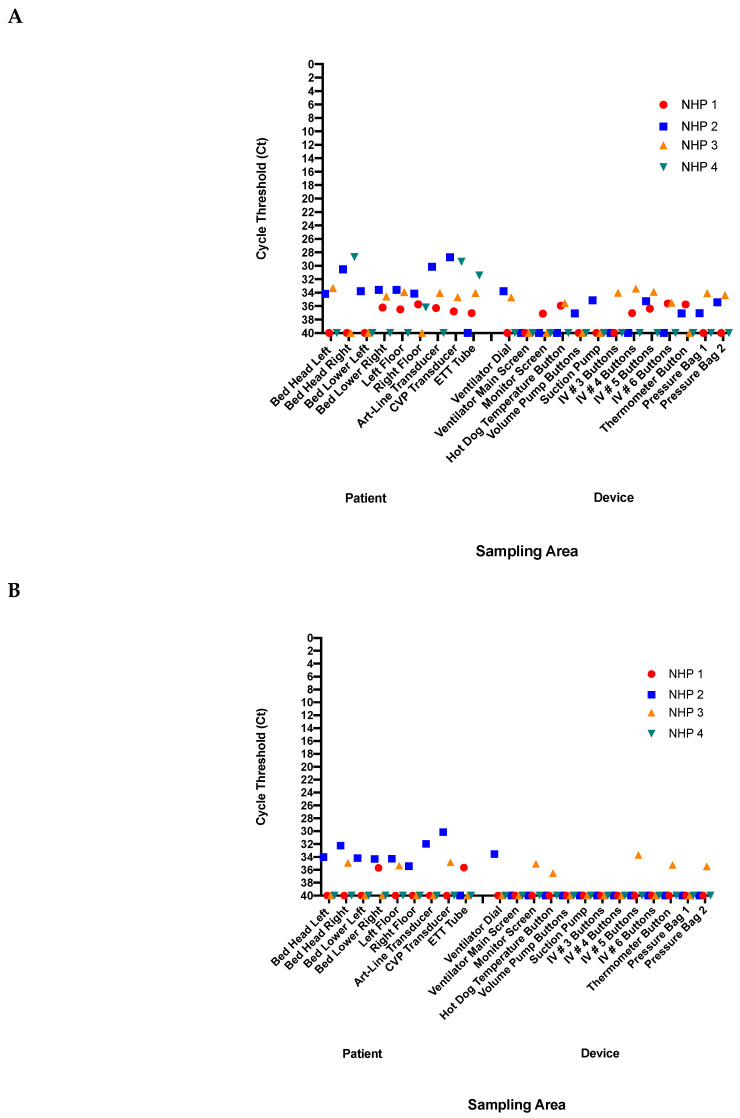
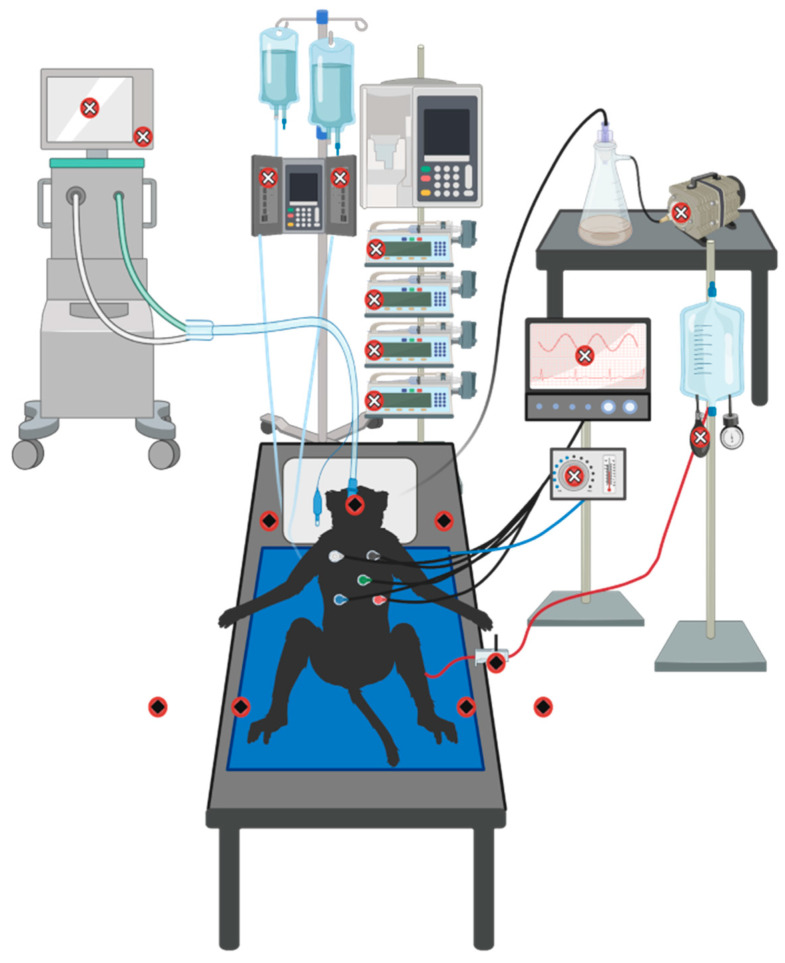
We created a fully equipped intensive care unit (ICU), within a Biosafety Level 4 (BSL4) laboratory, and infected multiple sedated non-human primates (NHPs) with Ebola virus. While providing bedside care, we sampled blood, urine, and gastric residuals; as well as buccal, ocular, nasal, rectal, and skin swabs, to assess the risks associated with routine care. We also assessed the physical environment at end-point.
Although viral RNA was detectable in blood as early as three days post-infection, it was not detectable in the urine, gastric fluid, or swabs until late-stage disease. While droplet spread and fomite contamination were present on a few of the surfaces that were routinely touched while providing care in the ICU for the infected animal, these may have been abrogated through good routine hygiene practices.
Overall this study has helped further our understanding of which procedures may pose the highest risk to healthcare providers and provides temporal evidence of this over the clinical course of disease.
2014 - 2016年西非埃博拉疫情再次表明,埃博拉病毒可在医院内传播,医护人员面临特别风险,包括欧洲和北美的显著病例。这些事件凸显了各中心更好地为潜在埃博拉病毒病例做准备的必要性;包括了解病毒如何传播以及哪些干预措施带来的风险最大。
我们在生物安全4级(BSL4)实验室中创建了一个设备齐全的重症监护病房(ICU),并用埃博拉病毒感染了多只镇静的非人灵长类动物(NHP)。在提供床边护理时,我们采集血液、尿液和胃内残余物样本;以及颊部、眼部、鼻部、直肠和皮肤拭子样本,以评估与常规护理相关的风险。我们还在终点时评估了物理环境。
虽然早在感染后三天就能在血液中检测到病毒RNA,但直到疾病晚期才在尿液、胃液或拭子中检测到。在为感染动物在ICU提供护理时,在一些经常接触的表面上存在飞沫传播和污染物污染,但通过良好的日常卫生习惯这些可能已被消除。
总体而言,本研究有助于进一步了解哪些程序可能对医护人员构成最高风险,并在疾病临床过程中提供了这方面的时间证据。