Triantafyllou Konstantinos, Gkolfakis Paraskevas, Skamnelos Alexandros, Diamantopoulou Georgia, Dagas Athanasios, Tziatzios Georgios, Thomopoulos Konstantinos, Potamianos Spyros, Christodoulou Dimitrios
Hepatogastroenterology Unit, Second Department of Internal Medicine - Propaedeutic, Research Institute and Diabetes Center, Medical School, National and Kapodistrian University of Athens, "Attikon" University General Hospital, Athens.
Division of Gastroenterology, University Hospital & Faculty of Medicine, School of Health Sciences, University of Ioannina, Ioannina, Greece.
Endosc Int Open. 2021 Mar;9(3):E378-E387. doi: 10.1055/a-1339-0913. Epub 2021 Feb 19.
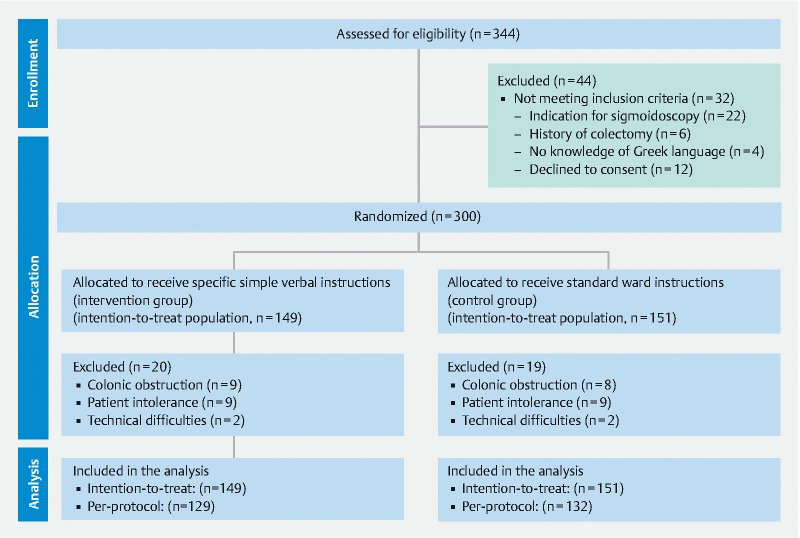
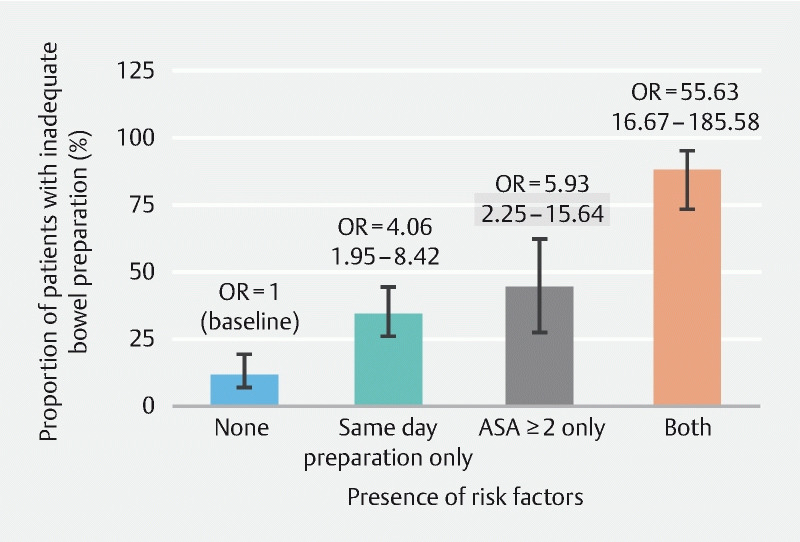
Bowel preparation for colonoscopy is frequently inadequate in hospitalized patients. We explored the impact of specific verbal instructions on the quality of inpatients bowel preparation and factors associated with preparation failure. Randomized (1:1), two strata (mobilized vs. bedridden; 3:2) trial of consecutive inpatients from four tertiary centers, who received either specific, verbal instructions or the standard of care (SOC) ward instructions about bowel preparation. The rate of adequate bowel preparation (Boston Bowel Preparation Score [BBPS] ≥ 6, no segment < 2) comprised the primary endpoint. Mean BBPS score, good (BBPS score ≥ 7, no segment score < 2) and excellent (BBPS = 9) were among secondary endpoints. We randomized 300 inpatients (180 mobile) aged 71.7 ± 15.1 years in the intervention (49.7 %) and SOC (50.3 %) groups, respectively. Overall, more patients in the intervention group achieved adequate bowel preparation, but this difference did not reach statistical significance neither in the intention-to-treat [90/149 (60.4 %) vs. 82/151 (54.3 %); = 0.29] nor in the per-protocol analysis [90/129 (69.8 %) vs. 82/132 (62.1 %); = 0.19]. Overall BBPS score did not differ statistical significantly in the two groups, but the provision of specific verbal instructions was associated with significant higher rates of good (58.1 % vs. 43.2 %; = 0.02) and excellent (31.8 % vs. 16.7 %; = 0.004) bowel preparation compared to the SOC group. Administration of same-day bowel preparation and patient American Society of Anesthesiologists score > 2 were identified as risk factors for inadequate bowel preparation. Provision of specific verbal instructions did not increase the rate of adequate bowel preparation in a population of mobilized and bedridden hospitalized patients.
住院患者结肠镜检查的肠道准备往往不充分。我们探讨了特定口头指导对住院患者肠道准备质量的影响以及与准备失败相关的因素。对来自四个三级中心的连续住院患者进行随机(1:1)、两个分层(可活动患者与卧床患者;3:2)试验,这些患者接受了关于肠道准备的特定口头指导或标准护理(SOC)病房指导。充分肠道准备率(波士顿肠道准备评分[BBPS]≥6,无节段<2)为主要终点。平均BBPS评分、良好(BBPS评分≥7,无节段评分<2)和优秀(BBPS = 9)为次要终点。我们分别将300名年龄为71.7±15.1岁的住院患者(180名可活动患者)随机分为干预组(49.7%)和SOC组(50.3%)。总体而言,干预组中更多患者实现了充分的肠道准备,但无论是在意向性分析[90/149(60.4%)对82/151(54.3%);P = 0.29]还是在符合方案分析[90/129(69.8%)对82/132(62.1%);P = 0.19]中,这种差异均未达到统计学意义。两组的总体BBPS评分在统计学上无显著差异,但与SOC组相比,提供特定口头指导与更高的良好(58.1%对43.2%;P = 0.02)和优秀(31.8%对16.7%;P = 0.004)肠道准备率相关。当日进行肠道准备以及患者美国麻醉医师协会评分>2被确定为肠道准备不充分的危险因素。在可活动和卧床住院患者群体中,提供特定口头指导并未提高充分肠道准备率。