Haouzi Philippe, McCann Marissa, Tubbs Nicole
Division of Pulmonary and Critical Care Medicine, Department of Medicine, Pennsylvania State University, College of Medicine, Hershey, Pennsylvania.
J Neurophysiol. 2021 Apr 1;125(4):1396-1407. doi: 10.1152/jn.00711.2020. Epub 2021 Mar 3.
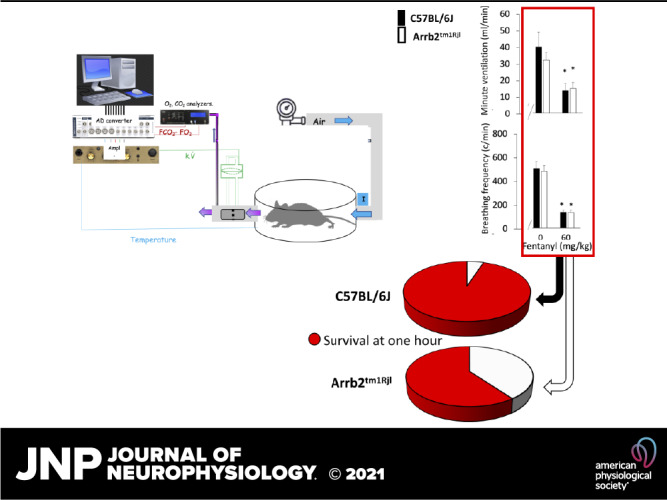
We have investigated the potential acute desensitizing role of the β arrestin 2 (β-arr2) pathway on the ventilatory depression produced by levels of fentanyl ranging from analgesic to life-threatening (0.1 to 60 mg/kg ip) in control and β-arr2-deficient nonsedated mice. Fentanyl at doses of 0.1, 0.5, and 1 mg/kg ip-corresponding to the doses previously used to study the role of β-arr2 pathway-decreased ventilation, but along the V̇e/V̇co relationship established in baseline conditions. This reduction in ventilation was therefore indistinguishable from the decrease in breathing during the periods of spontaneous immobility. Above 1.5 mg/kg, however, ventilation was depressed out of proportion of the changes in metabolic rate, suggesting a specific depression of the drive to breathe. The ventilatory responses were similar between the two groups. At high doses of fentanyl (60 mg/kg ip) 1 out of 20 control mice died by apnea versus 8 out of 20 β-arr2-deficient mice ( = 0.008). In the surviving mice, ventilation was however identical in both groups. The ventilatory effects of fentanyl in β-arr2-deficient mice, reported in the literature, are primarily mediated by the "indirect" effects of sedation/hypometabolism on breathing control. There was an excess mortality at very high doses of fentanyl in the β-arr2-deficient mice, mechanisms of which are still open to question, as the capacity of maintaining a rhythmic, although profoundly depressed, breathing activity remains similar in all of the surviving control and β-arr2-deficient mice. When life-threatening doses of fentanyl are used in mice, the β-arrestin 2 pathway appears to play a critical role in the recovery from opioid overdose. This observation calls into question the use of G protein-biased μ-opioid receptor agonists, as a strategy for safer opioid analgesic drugs.
我们研究了β抑制蛋白2(β-arr2)通路在对照和β-arr2基因缺陷的未镇静小鼠中,对芬太尼从镇痛剂量到危及生命剂量(腹腔注射0.1至60mg/kg)所产生的呼吸抑制的潜在急性脱敏作用。腹腔注射剂量为0.1、0.5和1mg/kg的芬太尼——与先前用于研究β-arr2通路作用的剂量相对应——可降低通气量,但符合基线条件下建立的每分通气量/二氧化碳排出量关系。因此,这种通气量的降低与自发不动期间呼吸的减少并无差异。然而,当剂量高于1.5mg/kg时,通气量的降低与代谢率的变化不成比例,提示呼吸驱动受到特异性抑制。两组的通气反应相似。腹腔注射高剂量芬太尼(60mg/kg)时,20只对照小鼠中有1只死于呼吸暂停,而20只β-arr2基因缺陷小鼠中有8只(P = 0.008)。然而,在存活的小鼠中,两组的通气情况相同。文献报道,芬太尼对β-arr2基因缺陷小鼠的通气作用主要由镇静/低代谢对呼吸控制的“间接”作用介导。在β-arr2基因缺陷小鼠中,使用极高剂量芬太尼时死亡率过高,其机制仍有待探讨,因为在所有存活的对照小鼠和β-arr2基因缺陷小鼠中,维持有节律的(尽管深度抑制)呼吸活动的能力仍然相似。当在小鼠中使用危及生命剂量的芬太尼时,β抑制蛋白2通路似乎在阿片类药物过量后的恢复中起关键作用。这一观察结果对使用G蛋白偏向性μ阿片受体激动剂作为更安全的阿片类镇痛药策略提出了质疑。