Nuffield Department of Primary Care Health Sciences, University of Oxford, Oxford, UK; Centre for Trials Research, School of Medicine, College of Biomedical and Life Sciences, Cardiff University, Cardiff, UK.
Nuffield Department of Primary Care Health Sciences, University of Oxford, Oxford, UK.
Br J Gen Pract. 2021 Mar 26;71(705):e266-e272. doi: 10.3399/BJGP.2020.0823. Print 2021 Apr.
C-reactive protein (CRP) point-of-care testing can reduce antibiotic use in patients with acute exacerbation of chronic obstructive pulmonary disease (AECOPD) in primary care, without compromising patient care. Further safe reductions may be possible.
To investigate the associations between presenting features and antibiotic prescribing in patients with AECOPD in primary care.
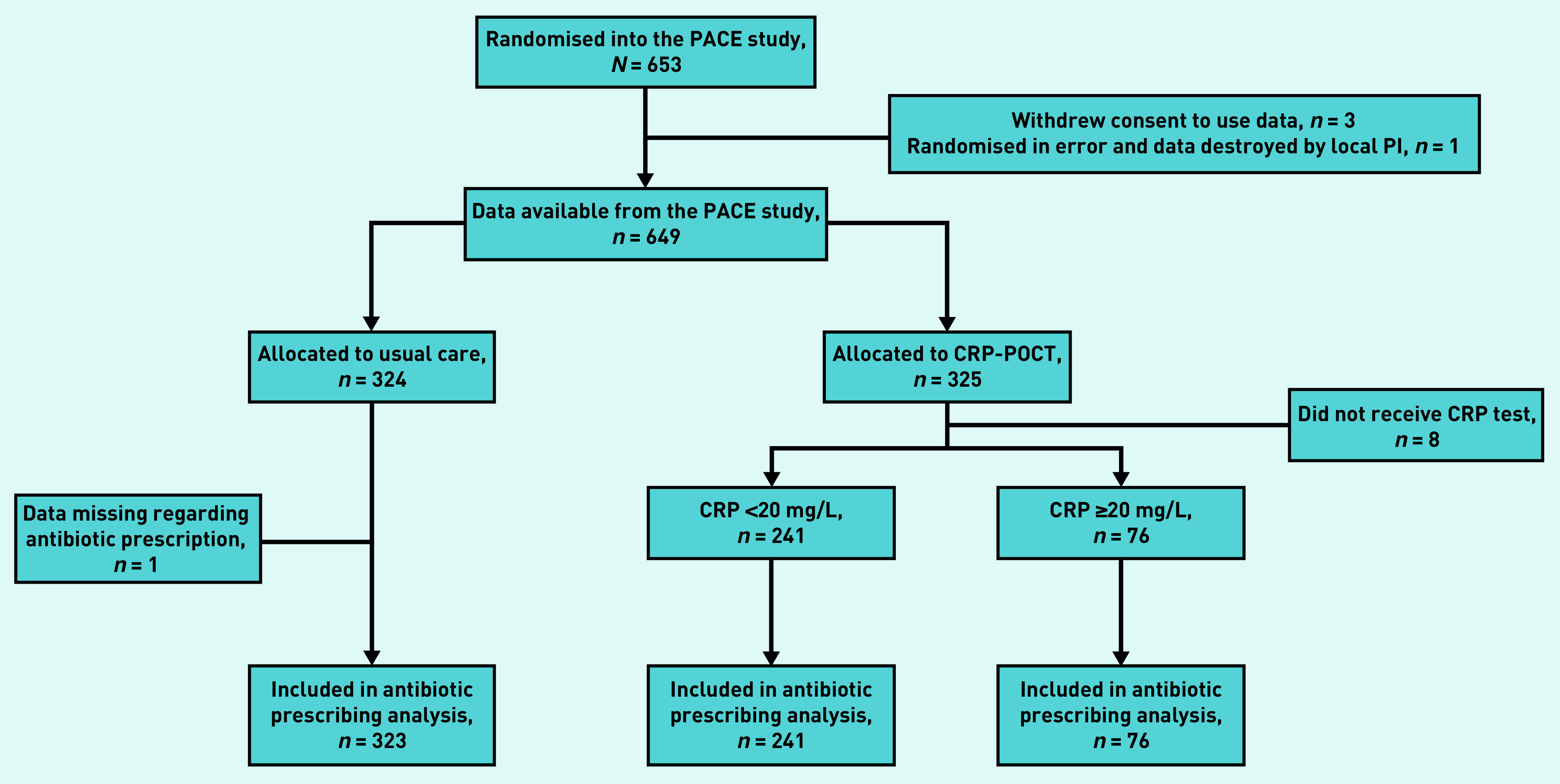
Secondary analysis of a randomised controlled trial of participants presenting with AECOPD in primary care (the PACE trial).
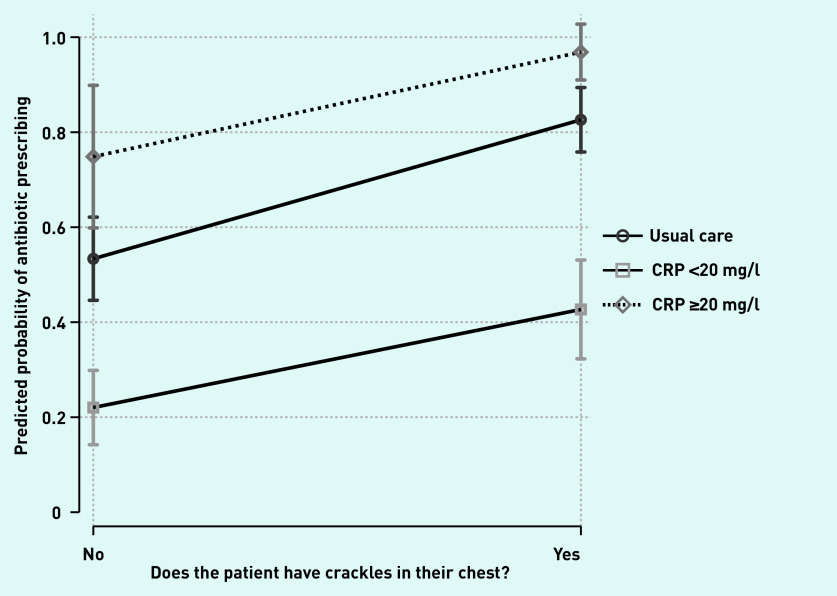
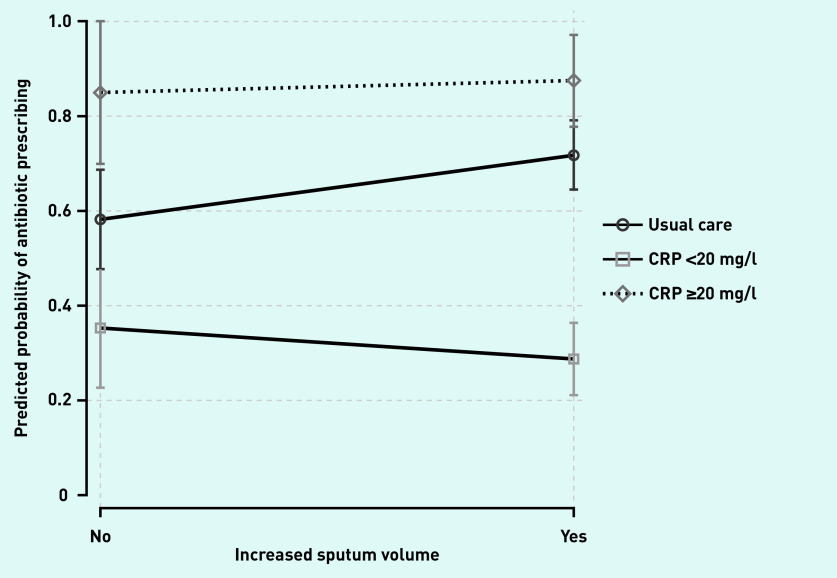
Clinicians collected participants' demographic features, comorbid illnesses, clinical signs, and symptoms. Antibiotic prescribing decisions were made after participants were randomised to receive a point-of-care CRP measurement or usual care. Multivariable regression models were fitted to explore the association between patient and clinical features and antibiotic prescribing, and extended to further explore any interactions with CRP measurement category (CRP not measured, CRP <20 mg/l, or CRP ≥20 mg/l).
A total of 649 participants from 86 general practices across England and Wales were included. Odds of antibiotic prescribing were higher in the presence of clinician-recorded crackles (adjusted odds ratio [AOR] = 5.22, 95% confidence interval [CI] = 3.24 to 8.41), wheeze (AOR = 1.64, 95% CI = 1.07 to 2.52), diminished vesicular breathing (AOR = 2.95, 95% CI = 1.70 to 5.10), or clinician-reported evidence of consolidation (AOR = 34.40, 95% CI = 2.84 to 417.27). Increased age was associated with lower odds of antibiotic prescribing (AOR per additional year increase = 0.98, 95% CI = 0.95 to 1.00), as was the presence of heart failure (AOR = 0.32, 95% CI = 0.12 to 0.85).
Several demographic features and clinical signs and symptoms are associated with antibiotic prescribing in AECOPD. Diagnostic and prognostic value of these features may help identify further safe reductions.
C 反应蛋白(CRP)即时检测可减少初级保健中慢性阻塞性肺疾病急性加重(AECOPD)患者的抗生素使用,而不会影响患者的护理。可能会进一步安全地减少抗生素的使用。
研究初级保健中 AECOPD 患者的临床表现与抗生素使用之间的关系。
对初级保健中 AECOPD 患者的一项随机对照试验(PACE 试验)进行二次分析。
临床医生收集参与者的人口统计学特征、合并症、临床体征和症状。在参与者被随机分配接受即时 CRP 测量或常规护理后,做出抗生素使用的决策。使用多变量回归模型来探索患者和临床特征与抗生素使用之间的关系,并进一步扩展到探索 CRP 测量类别(未测量 CRP、CRP<20mg/L 或 CRP≥20mg/L)的任何交互作用。
来自英格兰和威尔士 86 家全科诊所的 649 名参与者被纳入研究。临床医生记录的湿啰音(调整后的优势比 [OR] = 5.22,95%置信区间 [CI] = 3.24 至 8.41)、喘鸣(OR = 1.64,95% CI = 1.07 至 2.52)、呼吸音减弱(OR = 2.95,95% CI = 1.70 至 5.10)或临床医生报告的实变证据存在时,抗生素使用的可能性更高(OR = 34.40,95% CI = 2.84 至 417.27)。年龄每增加一年,抗生素使用的可能性降低(每增加一年的调整后 OR = 0.98,95% CI = 0.95 至 1.00),心力衰竭的存在也与抗生素使用的可能性降低相关(OR = 0.32,95% CI = 0.12 至 0.85)。
一些人口统计学特征和临床体征和症状与 AECOPD 中的抗生素使用有关。这些特征的诊断和预后价值可能有助于进一步确定安全的减少。