Broers Merel C, Bunschoten Carina, Drenthen Judith, Beck Tiago A O, Brusse Esther, Lingsma Hester F, Allen Jeffrey A, Lewis Richard A, van Doorn Pieter A, Jacobs Bart C
Department of Neurology, Erasmus MC, University Medical Center Rotterdam, Rotterdam, The Netherlands.
Department of Clinical Neurophysiology, Erasmus MC, University Medical Center Rotterdam, Rotterdam, The Netherlands.
Eur J Neurol. 2021 Jun;28(6):2065-2073. doi: 10.1111/ene.14796. Epub 2021 Apr 9.
The aim of this study was to determine the frequency of over- and underdiagnosis of chronic inflammatory demyelinating polyradiculoneuropathy (CIDP) and to identify related diagnostic pitfalls.
We conducted a retrospective study in Dutch patients referred to the Erasmus University Medical Centre Rotterdam between 2011 and 2017 with either a diagnosis of CIDP or another diagnosis that was revised to CIDP. We used the European Federation of Neurological Societies/Peripheral Nerve Society (EFNS/PNS) 2010 diagnostic criteria for CIDP to classify patients into three groups: overdiagnosis, underdiagnosis, or confirmed diagnosis of CIDP. Clinical and laboratory features and treatment history were compared between groups.
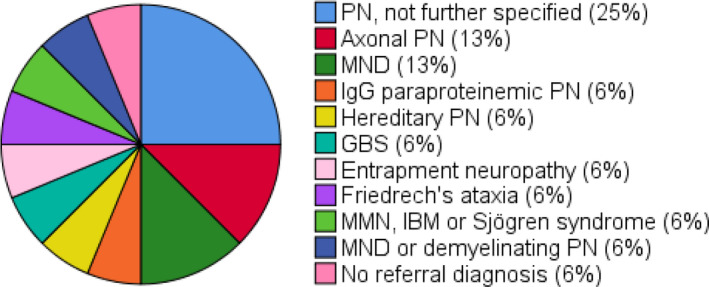
A referral diagnosis of CIDP was revised in 32% of patients (31/96; overdiagnosis). Of 81 patients diagnosed with CIDP, 16 (20%) were referred with another diagnosis (underdiagnosis). In the overdiagnosed patients, 20% of muscle weakness was asymmetric, 48% lacked proximal muscle weakness, 29% only had distal muscle weakness, 65% did not fulfil the electrodiagnostic criteria for CIDP, 74% had an elevated cerebrospinal fluid (CSF) protein level, and 97% had another type of neuropathy. In the underdiagnosed patients, all had proximal muscle weakness, 50% had a clinically atypical CIDP, all fulfilled the electrodiagnostic criteria for CIDP, and 25% had an increased CSF protein level.
Over- and underdiagnosis of CIDP is common. Diagnostic pitfalls include lack of attention to proximal muscle weakness as a diagnostic hallmark of CIDP, insufficient recognition of clinical atypical phenotypes, overreliance on CSF protein levels, misinterpretation of nerve conduction studies and poor adherence to electrodiagnostic criteria, and failure to exclude other causes of polyneuropathy.
本研究旨在确定慢性炎症性脱髓鞘性多发性神经根神经病(CIDP)过度诊断和诊断不足的频率,并识别相关的诊断陷阱。
我们对2011年至2017年间转诊至鹿特丹伊拉斯姆斯大学医学中心的荷兰患者进行了一项回顾性研究,这些患者要么被诊断为CIDP,要么最初诊断为其他疾病,后来修订为CIDP。我们使用欧洲神经病学学会联合会/外周神经学会(EFNS/PNS)2010年CIDP诊断标准将患者分为三组:过度诊断、诊断不足或确诊为CIDP。比较了各组之间的临床和实验室特征以及治疗史。
32%的患者(31/96)最初诊断为CIDP后被修订(过度诊断)。在81例诊断为CIDP的患者中,16例(20%)最初被诊断为其他疾病(诊断不足)。在过度诊断的患者中,20%的肌无力为不对称性,48%缺乏近端肌无力,29%仅存在远端肌无力,65%不符合CIDP的电诊断标准,74%脑脊液(CSF)蛋白水平升高,97%患有其他类型的神经病。在诊断不足的患者中,均有近端肌无力,50%具有临床非典型CIDP,均符合CIDP的电诊断标准,25%脑脊液蛋白水平升高。
CIDP的过度诊断和诊断不足很常见。诊断陷阱包括未将近端肌无力作为CIDP的诊断标志予以重视、对临床非典型表型认识不足、过度依赖CSF蛋白水平、对神经传导研究的错误解读以及未严格遵循电诊断标准,还有未能排除多发性神经病的其他病因。