Department of Hematological medicine, King's College Hospital, London, UK.
Hematology, Fondazione IRCCS Ca' Granda Ospedale Maggiore Policlinico di Milano, Milan, Italy.
Leukemia. 2021 Nov;35(11):3223-3231. doi: 10.1038/s41375-021-01190-9. Epub 2021 Mar 4.
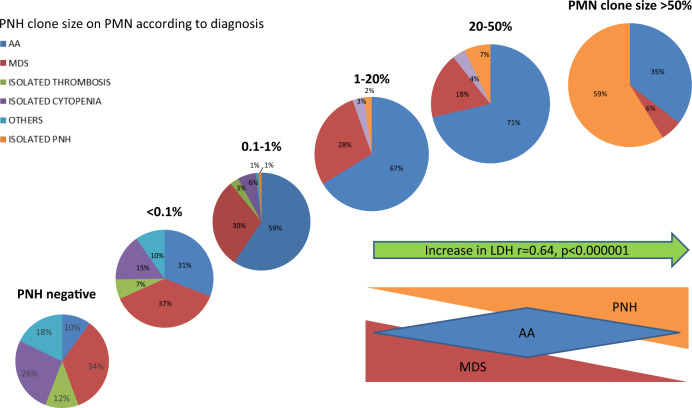
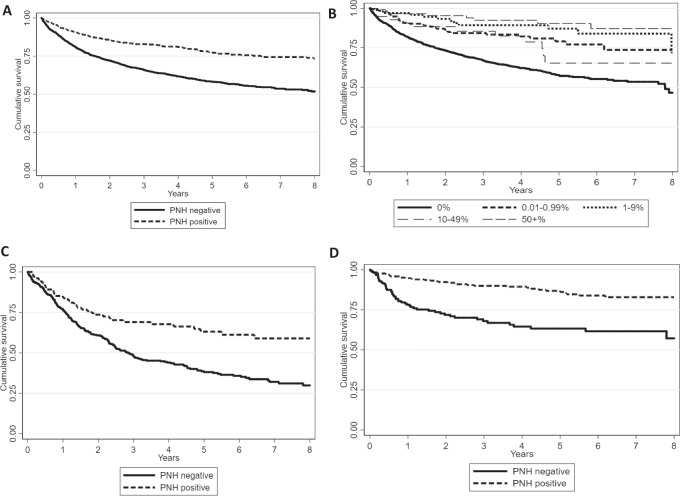
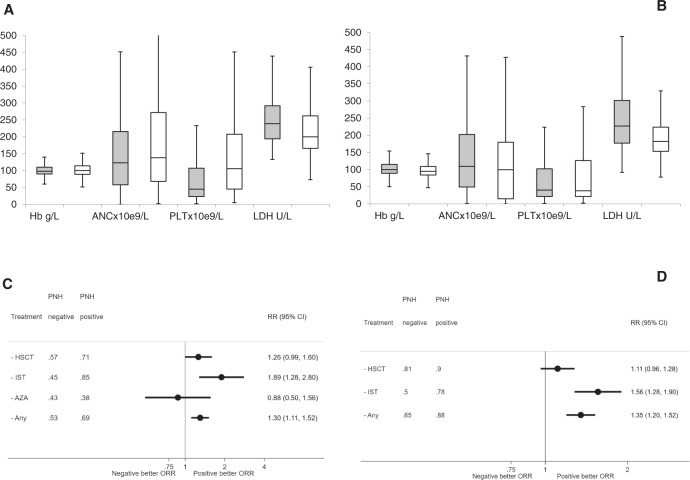
In this large single-centre study, we report high prevalence (25%) of, small (<10%) and very small (<1%), paroxysmal nocturnal hemoglobinuria (PNH) clones by high-sensitive cytometry among 3085 patients tested. Given PNH association with bone marrow failures, we analyzed 869 myelodysplastic syndromes (MDS) and 531 aplastic anemia (AA) within the cohort. PNH clones were more frequent and larger in AA vs. MDS (p = 0.04). PNH clone, irrespective of size, was a good predictor of response to immunosuppressive therapy (IST) and to stem cell transplant (HSCT) (in MDS: 84% if PNH+ vs. 44.7% if PNH-, p = 0.01 for IST, and 71% if PNH+ vs. 56.6% if PNH- for HSCT; in AA: 78 vs. 50% for IST, p < 0.0001, and 97 vs. 77%, p = 0.01 for HSCT). PNH positivity had a favorable impact on disease progression (0.6% vs. 4.9% IPSS-progression in MDS, p < 0.005; and 2.1 vs. 6.9% progression to MDS in AA, p = 0.01), leukemic evolution (6.8 vs. 12.7%, p = 0.01 in MDS), and overall survival [73% (95% CI 68-77) vs. 51% (48-54), p < 0.0001], with a relative HR for mortality of 2.37 (95% CI 1.8-3.1; p < 0.0001) in PNH negative cases, both in univariate and multivariable analysis. Our data suggest systematic PNH testing in AA/MDS, as it might allow better prediction/prognostication and consequent clinical/laboratory follow-up timing.
在这项大型单中心研究中,我们报告了在 3085 名检测患者中,通过高敏感细胞术检测到阵发性夜间血红蛋白尿 (PNH) 克隆的高发生率 (25%),且克隆较小 (<10%) 和非常小 (<1%)。鉴于 PNH 与骨髓衰竭有关,我们在该队列中分析了 869 例骨髓增生异常综合征 (MDS) 和 531 例再生障碍性贫血 (AA)。与 MDS 相比,AA 中 PNH 克隆更频繁且更大 (p=0.04)。无论大小如何,PNH 克隆都是免疫抑制治疗 (IST) 和干细胞移植 (HSCT) 反应的良好预测指标 (在 MDS 中:PNH+的 84% vs. PNH-的 44.7%,IST 的 p=0.01,PNH+的 71% vs. PNH-的 56.6%,HSCT 的 p=0.01)。在 AA 中:IST 的 78% vs. 50%,p<0.0001,HSCT 的 97% vs. 77%,p=0.01)。PNH 阳性对疾病进展有有利影响 (MDS 中 IPSS 进展的 0.6% vs. 4.9%,p<0.005;AA 中进展为 MDS 的 2.1% vs. 6.9%,p=0.01)、白血病演变 (6.8% vs. 12.7%,p=0.01 在 MDS 中) 和总生存 [73% (95% CI 68-77) vs. 51% (48-54),p<0.0001],PNH 阴性病例的死亡相对风险为 2.37 (95% CI 1.8-3.1;p<0.0001),在单因素和多因素分析中均如此。我们的数据表明,在 AA/MDS 中应系统地进行 PNH 检测,因为它可能允许更好地预测/预后,并相应地调整临床/实验室随访时间。