Division of Medicine, Centre for Rheumatology and Clinical Immunology, Turku University Hospital.
Department of Medicine, University of Turku, Turku.
Rheumatology (Oxford). 2021 Nov 3;60(11):5205-5215. doi: 10.1093/rheumatology/keab204.
To investigate the long-term outcomes of patients with RA after myocardial infarction (MI).
All-comer, real-life MI patients with RA (n = 1614, mean age 74 years) were retrospectively compared with propensity score (1:5) matched MI patients without RA (n = 8070) in a multicentre, nationwide, cohort register study in Finland. The impact of RA duration and the usage of corticosteroids and antirheumatic drugs on RA patients' outcomes were also studied. The median follow-up was 7.3 years.
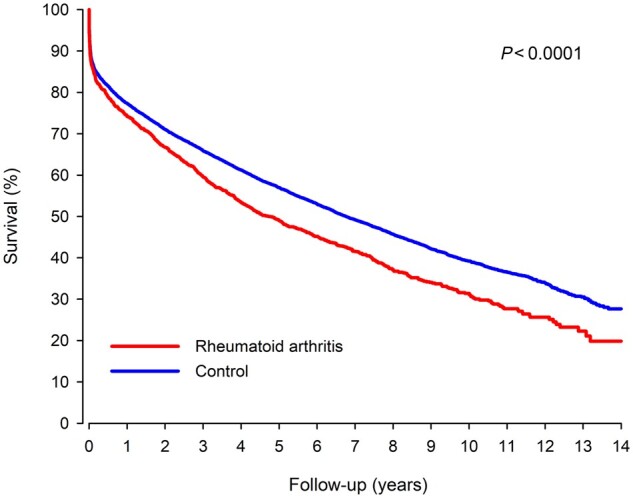
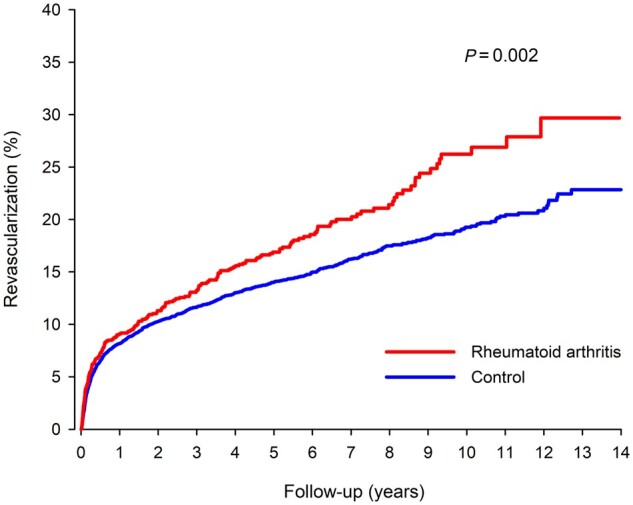
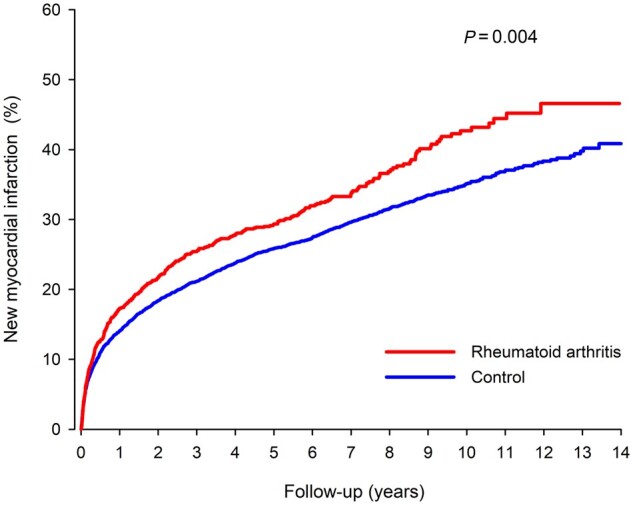
RA was associated with an increased 14-year mortality risk after MI compared with patients without RA [80.4% vs 72.3%; hazard ratio (HR) 1.25; CI: 1.16, 1.35; P <0.0001]. Patients with RA were at higher risk of new MI (HR 1.22; CI: 1.09, 1.36; P =0.0001) and revascularization (HR 1.28; CI: 1.10, 1.49; P =0.002) after discharge from index MI. Cumulative stroke rate after MI did not differ between RA and non-RA patients (P =0.322). RA duration and corticosteroid usage before MI, but not use of methotrexate or biologic antirheumatic drugs, were independently associated with higher mortality (P <0.001) and new MI (P =0.009). A higher dosage of corticosteroids prior to MI was independently associated with higher long-term mortality (P =0.002) and methotrexate usage with lower stroke rate (P =0.034). Serological status of RA was not associated with outcomes.
RA is independently associated with poorer prognosis after MI. RA duration and corticosteroid usage and dosage were independent predictors of mortality after MI in RA. Special attention is needed for improvement of outcomes after MI in this vulnerable population.
研究心肌梗死后类风湿关节炎(RA)患者的长期结局。
在芬兰一项多中心、全国性的队列登记研究中,回顾性比较了所有接受治疗的心肌梗死后伴 RA(n=1614,平均年龄 74 岁)和不伴 RA 的心肌梗死患者(n=8070),并采用倾向评分(1:5)进行匹配。还研究了 RA 持续时间以及皮质类固醇和抗风湿药物的使用对 RA 患者结局的影响。中位随访时间为 7.3 年。
与无 RA 患者相比,RA 患者心肌梗死后 14 年的死亡率风险增加[80.4%比 72.3%;风险比(HR)1.25;95%CI:1.16,1.35;P<0.0001]。RA 患者发生新发心肌梗死(HR 1.22;95%CI:1.09,1.36;P=0.0001)和血运重建(HR 1.28;95%CI:1.10,1.49;P=0.002)的风险更高。MI 后,RA 患者的累积卒中发生率与非 RA 患者无差异(P=0.322)。MI 前的 RA 持续时间和皮质类固醇使用与较高的死亡率(P<0.001)和新发心肌梗死(P=0.009)独立相关,但甲氨蝶呤或生物抗风湿药物的使用与死亡率或新发心肌梗死无关。MI 前皮质类固醇的剂量与长期死亡率独立相关(P=0.002),而甲氨蝶呤的使用与较低的卒中率独立相关(P=0.034)。RA 的血清学状态与结局无关。
RA 与 MI 后预后不良独立相关。RA 持续时间、皮质类固醇使用和剂量是 MI 后 RA 患者死亡的独立预测因素。在这一脆弱人群中,需要特别注意改善 MI 后的结局。