de Winkel Jordi, van der Jagt Mathieu, Lingsma Hester F, Roozenbeek Bob, Calvillo Eusebia, Chou Sherry H-Y, Dziedzic Peter H, Etminan Nima, Huang Judy, Ko Nerissa U, Loch MacDonald Robert, Martin Renee L, Potu Niteesh R, Venkatasubba Rao Chethan P, Vergouwen Mervyn D I, Suarez Jose I
Department of Neurology, Erasmus MC, University Medical Center Rotterdam, 3000 CA Rotterdam, The Netherlands.
Department of Public Health, Erasmus MC, University Medical Center Rotterdam, 3000 CA Rotterdam, The Netherlands.
J Clin Med. 2021 Feb 14;10(4):762. doi: 10.3390/jcm10040762.
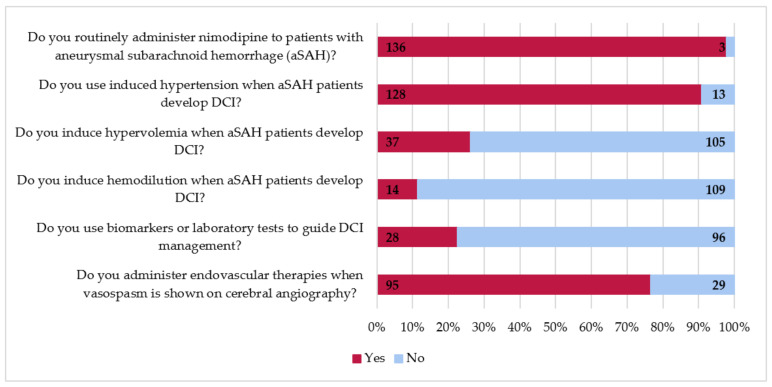
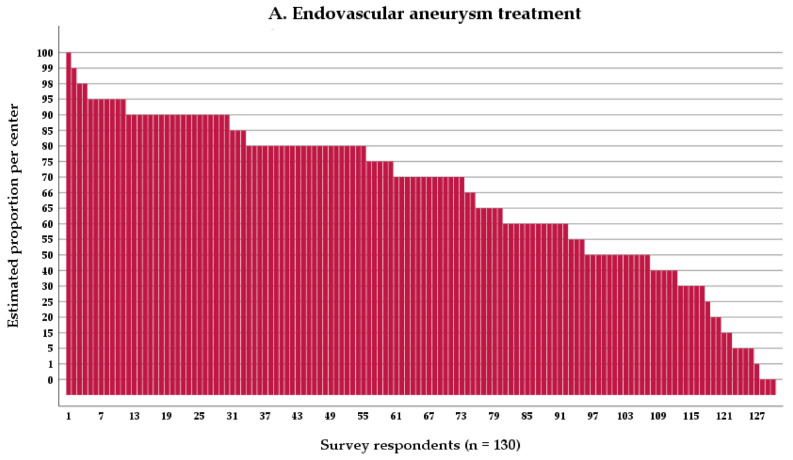
Prior research suggests substantial between-center differences in functional outcome following aneurysmal subarachnoid hemorrhage (aSAH). One hypothesis is that these differences are due to practice variability. To characterize practice variability, we sent a survey to 230 centers, of which 145 (63%) responded. Survey respondents indicated that an estimated 65% of ruptured aneurysms were treated endovascularly. Sixty-five percent of aneurysms were treated within 24 h of symptom onset, 18% within 24-48 h, and eight percent within 48-72 h. Centers in the United States (US) and Europe (EU) treat aneurysms more often endovascularly (72% and 70% vs. 51%, respectively, US vs. other < 0.001, and EU vs. other < 0.01) and more often within 24 h (77% and 64% vs. 46%, respectively, US vs. other < 0.001, EU vs. other < 0.01) compared to other centers. Most centers aim for euvolemia (96%) by administrating intravenous fluids to 0 (53%) or +500 mL/day (41%) net fluid balance. Induced hypertension is more often used in US centers (100%) than in EU (87%, < 0.05) and other centers (81%, < 0.05), and endovascular therapies for cerebral vasospasm are used more often in US centers than in other centers (91% and 60%, respectively, < 0.05). We observed significant practice variability in aSAH treatment worldwide. Future comparative effectiveness research studies are needed to investigate how practice variation leads to differences in functional outcome.
先前的研究表明,动脉瘤性蛛网膜下腔出血(aSAH)后功能结局在各中心之间存在显著差异。一种假设是,这些差异是由于实践的变异性所致。为了描述实践的变异性,我们向230个中心发送了一份调查问卷,其中145个中心(63%)进行了回复。参与调查的受访者表示,估计65%的破裂动脉瘤采用血管内治疗。65%的动脉瘤在症状发作后24小时内接受治疗,18%在24 - 48小时内接受治疗,8%在48 - 72小时内接受治疗。美国(US)和欧洲(EU)的中心相比其他中心更常采用血管内治疗动脉瘤(分别为72%和70%,而其他地区为51%,美国与其他地区相比P<0.001,欧盟与其他地区相比P<0.01),且更常在24小时内进行治疗(分别为77%和64%,而其他地区为46%,美国与其他地区相比P<0.001,欧盟与其他地区相比P<0.01)。大多数中心通过给予静脉输液使净液体平衡为0(53%)或+500毫升/天(41%)来实现血容量正常(96%)。美国中心比欧盟(87%,P<0.05)和其他中心(81%,P<0.05)更常使用诱导性高血压,并且美国中心比其他中心更常使用脑血管痉挛的血管内治疗(分别为91%和60%,P<0.05)。我们观察到全球范围内aSAH治疗存在显著的实践变异性。未来需要进行比较疗效研究,以调查实践差异如何导致功能结局的不同。