Pichler Renate, Lindner Andrea Katharina, Schäfer Georg, Tulchiner Gennadi, Staudacher Nina, Mayr Martin, Comperat Eva, Orme Jacob J, Schachtner Gert, Thurnher Martin
Department of Urology, Medical University of Innsbruck, 6020 Innsbruck, Austria.
Department of Pathology, Medical University of Innsbruck, 6020 Innsbruck, Austria.
J Clin Med. 2021 Feb 14;10(4):764. doi: 10.3390/jcm10040764.
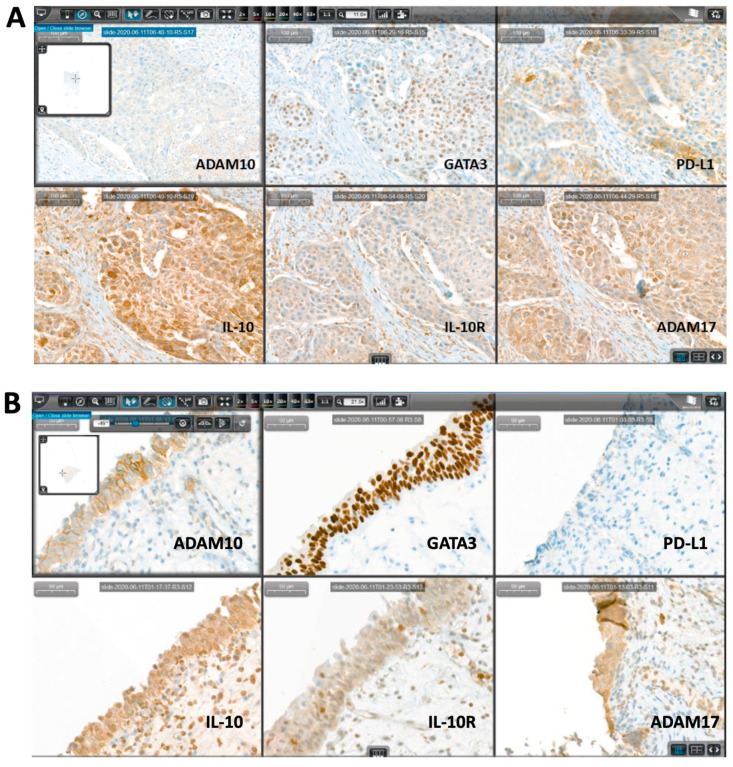
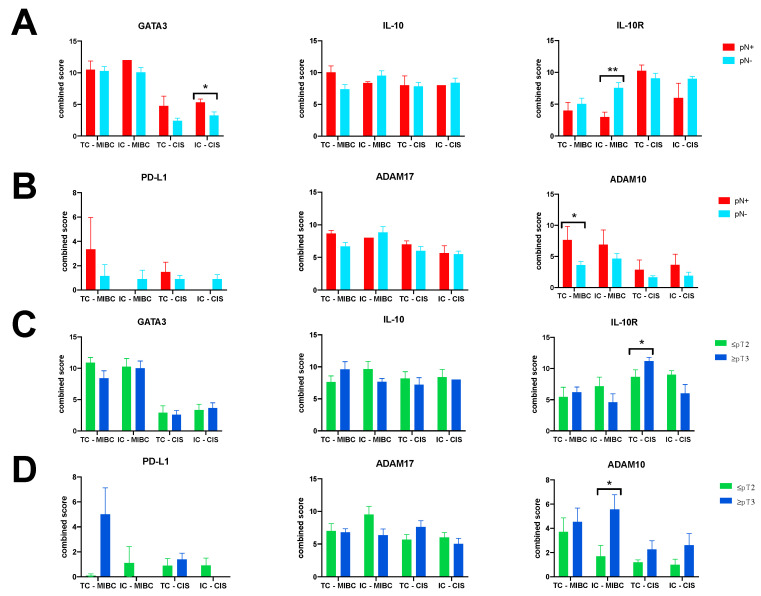
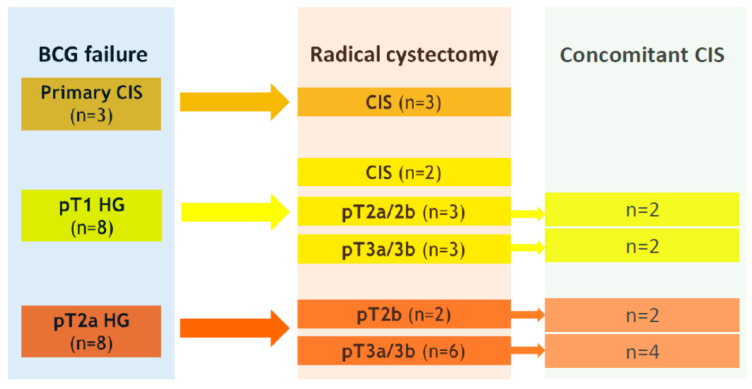
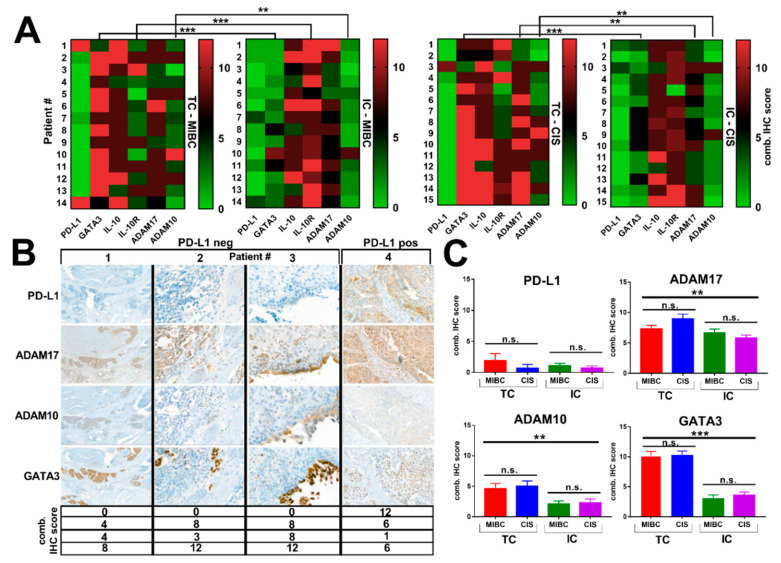
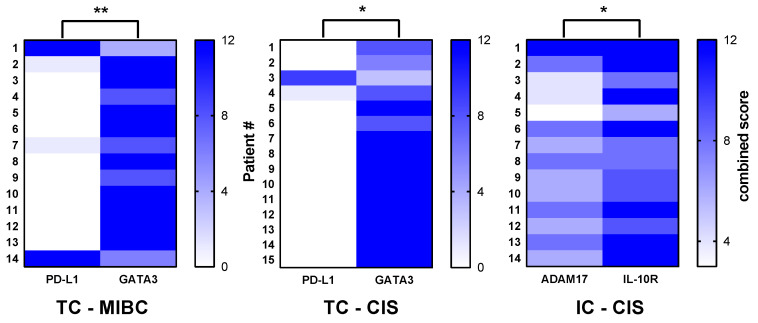
Although Bacillus Calmette Guérin (BCG) remains a mainstay of adjuvant treatment in high-risk, non-muscle-invasive bladder cancer, BCG failure occurs in up to 40% of patients, with radical cystectomy (RC) as the inevitable therapeutic consequence. Current data suggest that PD-L1 immunosuppressive signaling is responsible for BCG failure, supporting the therapeutic rationale of combining checkpoint inhibitors with BCG. To address the immune cascade in 19 RC specimens obtained after BCG failure, we applied a small immunohistochemical (IHC) panel consisting of selected markers (PD-L1, GATA-3, a disintegrin and metalloproteinase (ADAM) proteases, IL-10/IL-10R). A modified quick score was used for IHC semi-quantification of these markers in tumor cells (TC) and immune cells (IC) within two different regions: muscle-invasive bladder cancer (MIBC) and primary/concurrent carcinoma in situ (CIS). Contrary to expectation, PD-L1 was consistently low, irrespective of tumor region and cell type. Intriguingly, expression of ADAM17, which has been reported to release membrane-bound PD-L1, was high in both tumor regions and cell types. Moreover, expression of GATA3, IL-10, and IL-10R was also increased, indicative of a generally immunosuppressive tumor microenvironment in BCG failure. ADAM10 expression was associated with advanced tumor disease at RC. Our findings raise the possibility that ADAM proteases may cleave PD-L1 from the surface of bladder TC and possibly also from IC. Therefore, IHC assessment of PD-L1 expression seems to be insufficient and should be supplemented by ADAM10/17 in patients with BCG failure.
尽管卡介苗(BCG)仍是高危非肌层浸润性膀胱癌辅助治疗的主要手段,但高达40%的患者会出现BCG治疗失败,最终不可避免地需要进行根治性膀胱切除术(RC)。目前的数据表明,PD-L1免疫抑制信号是BCG治疗失败的原因,这支持了将检查点抑制剂与BCG联合使用的治疗原理。为了研究BCG治疗失败后获得的19个RC标本中的免疫级联反应,我们应用了一个小型免疫组织化学(IHC)检测组合,包括选定的标志物(PD-L1、GATA-3、解整合素和金属蛋白酶(ADAM)蛋白酶、IL-10/IL-10R)。采用改良的快速评分法对肿瘤细胞(TC)和免疫细胞(IC)中这些标志物在两个不同区域(肌层浸润性膀胱癌(MIBC)和原发性/同时性原位癌(CIS))进行IHC半定量分析。与预期相反,无论肿瘤区域和细胞类型如何,PD-L1始终较低。有趣的是,据报道可释放膜结合型PD-L1的ADAM17在两个肿瘤区域和细胞类型中的表达均较高。此外,GATA3、IL-10和IL-10R的表达也增加,表明BCG治疗失败时肿瘤微环境普遍具有免疫抑制作用。ADAM10的表达与RC时的晚期肿瘤疾病相关。我们的研究结果提示,ADAM蛋白酶可能从膀胱TC表面以及可能也从IC表面切割PD-L1。因此,对于BCG治疗失败的患者,IHC评估PD-L1表达似乎并不充分,应补充ADAM10/17检测。