Buranupakorn Tassaya, Thangsuk Phaviga, Patumanond Jayanton, Phinyo Phichayut
Department of Family Medicine, Chiang Rai Prachanukroh Hospital, Chiang Rai 57000, Thailand.
Center for Clinical Epidemiology and Clinical Statistics, Faculty of Medicine, Chiang Mai University, Chiang Mai 50200, Thailand.
Cancers (Basel). 2021 Feb 27;13(5):992. doi: 10.3390/cancers13050992.
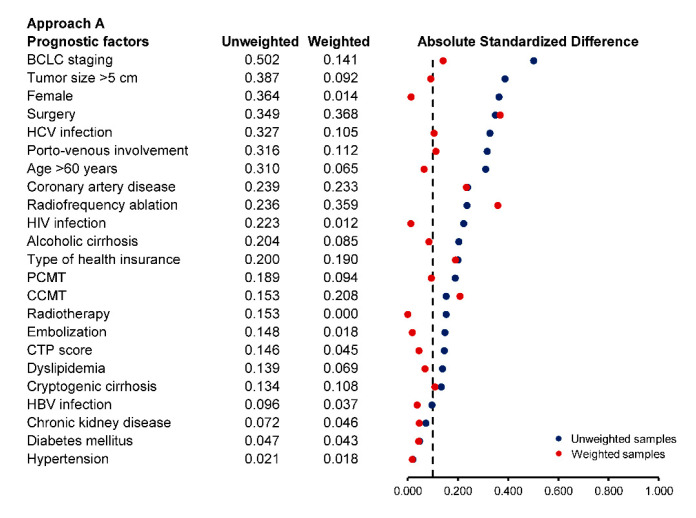
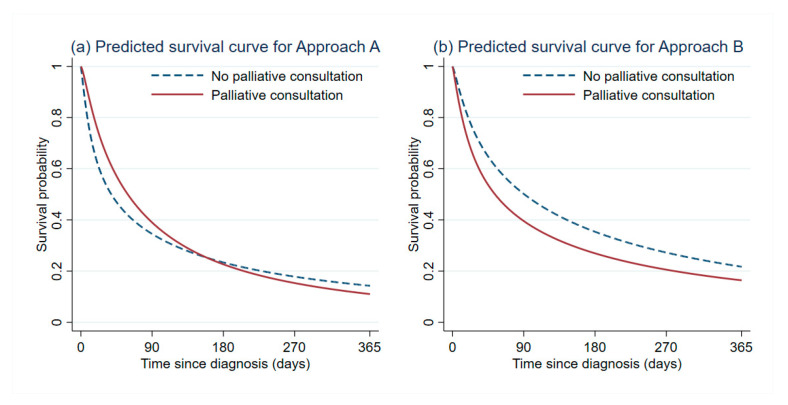
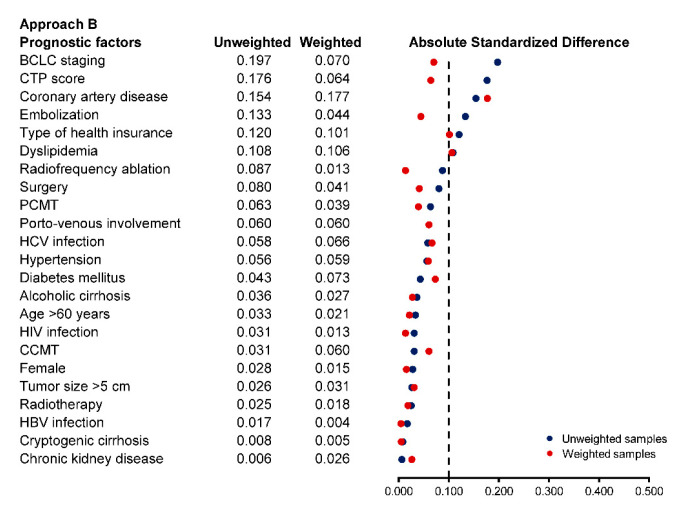
Palliative care has the potential to improve the quality of life of patients with incurable diseases or cancer, such as hepatocellular carcinoma (HCC). A common misconception of palliative care with respect to the patient's survival remains a significant barrier to the discipline. This study aimed to provide causal evidence for the effect of palliative care consultation on the survival time after diagnosis among HCC patients. An emulation of a target trial was conducted on a retrospective cohort of HCC patients from January 2017 to August 2019. The primary endpoint was the restricted mean survival time (RMST) at 12 months after HCC diagnosis. We used the clone-censor-weight approach to account for potential immortal time bias. In this study, 86 patients with palliative care consultation and 71 patients without palliative care consultation were included. The adjusted RMST difference was -29.7 (95% confidence interval (CI): -81.7, 22.3; -value = 0.263) days in favor of no palliative care consultation. However, palliative care consultation was associated with an increase in the prescription of symptom control medications, as well as a reduction in life-sustaining interventions and healthcare costs. Our findings suggest that palliative care consultation was associated with neither additional survival benefit nor harm in HCC patients. The misconception that it significantly accelerates the dying process should be disregarded.
姑息治疗有潜力改善患有不治之症或癌症(如肝细胞癌(HCC))患者的生活质量。对于患者生存而言,对姑息治疗的一个常见误解仍然是该学科的一个重大障碍。本研究旨在为姑息治疗会诊对HCC患者诊断后生存时间的影响提供因果证据。对2017年1月至2019年8月的HCC患者回顾性队列进行了目标试验模拟。主要终点是HCC诊断后12个月的受限平均生存时间(RMST)。我们使用克隆删失加权法来考虑潜在的不朽时间偏倚。本研究纳入了86例接受姑息治疗会诊的患者和71例未接受姑息治疗会诊的患者。调整后的RMST差异为-29.7天(95%置信区间(CI):-81.7,22.3;P值 = 0.263),有利于未接受姑息治疗会诊的患者。然而,姑息治疗会诊与症状控制药物处方的增加、维持生命干预措施的减少以及医疗费用的降低相关。我们的研究结果表明,姑息治疗会诊对HCC患者既无额外的生存益处也无危害。那种认为它会显著加速死亡过程的误解应该被摒弃。